
Abstract
Purpose
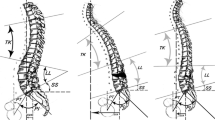
A decompensated sagittal imbalance has been associated with worsening health-related quality of life outcomes and increasing pain. Significant improvement in sagittal balance can be achieved using a pedicle subtraction osteotomy (PSO); however, this procedure has a high complication profile. A lumbar PSO has the advantages of direct visualization of all neural structures and safer retraction of the thecal sac. Sacrificing neuromonitoring may reduce anaesthesia time and lead to improved cost effectiveness of the surgery. However, there are no studies analyzing the complication rate of lumbar PSO without the use of neuromonitoring. We hypothesize that the neurologic complication rate remains comparable to published studies even without the use of intraoperative neuromonitoring.
Methods
The medical records of all patients of a single institution who received a lumbar PSO for sagittal imbalance between July 2012 and June 2014 were retrospectively analyzed. All surgeries were performed by the first author and without the use of intraoperative neuromonitoring. We analyzed the 30-day complication rate.
Results
Twenty-two patients were included in this study. The average age at surgery was 67 years. 16 patients had at least one previous lumbar surgery. The average fusion length was seven segments. All patients were instrumented to the sacrum and 19 patients additionally received spinopelvic instrumentation. The average amount of focal correction was 28°. The average surgical time was 362 min and blood loss was 2302 mL. A total of eight patients with complications were identified. There was a new neurologic postoperative deficit in two patients presenting as a foot drop. Five patients had an unplanned revision surgery.
Conclusion
Historically, PSOs are associated with a high surgical complication rate and our results show comparable outcomes and complications to those previously reported. In our series, the absence of neuromonitoring in lumbar PSOs does not appear to increase the risk of neurological injury.
Similar content being viewed by others


References
Vitale MG, Skaggs DL, Pace GI et al (2014) Best practice in intraoperative neuromonitoring in spine deformity surgery: development of an intraoperative checklist to optimize response. Spine Deform 2:333–339
Thuet ED, Winscher JC, Padberg AM et al (2010) Validity and reliability of intraoperative monitoring in pediatric spinal deformity surgery: a 23-year experience of 3436 surgical cases. Spine 35:1880–1886
Pahys JM, Guille JT, D’Andrea LP et al (2009) Neurologic injury in the surgical treatment of idiopathic scoliosis: guidelines for assessment and management. J Am Acad Orthop Surg 17:426–434
Pastorelli F, Si Silvestre M, Plasmati R et al (2011) The prevention of neural complications in the surgical treatment of scoliosis: the role of the neurophysiological intraoperative monitoring. Eur Spine J 20(Suppl 1):S105–S114
Kamerlink JR, Errico T, Xavier S et al (2010) Major intraoperative neurologic monitoring deficits in consecutive pediatric and adult spinal deformity patients a tone institution. Spine 35:240–245
Auerbach JD, Lenke LG, Bridwell KH et al (2012) Major complications and comparison between 3-column osteotomy techniques in 105 consecutive spinal deformity procedures. Spine 37:1198–1210
Hassanzadeh H, Jain A, El Dafrawy MH et al (2013) Three-column osteotomies in the treatment of spinal deformity in adult patients 60 years old and older: outcome and complications. Spine 38:726–731
Kelly MP, Lenke LG, Shaffrey CI et al (2014) Evaluation of complications and neurological deficits with three-column spine reconstructions for complex spinal deformity: a retrospective Scoli-RISK-1 study. Neurosurg Focus 36:E17
Ames CP, Barry JJ, Keshavarzi S et al (2013) Perioperative outcomes and complications of pedicle subtraction osteotomy in cases with single versus two attending surgeons. Spine Deform 1:51–58
Buchowski JM, Bridwell KH, Lenke LG et al (2007) Neurologic complications of lumbar pedicle subtraction osteotomy: a 10-year assessment. Spine 32:2245–2252
McCarthy IM, Hostin RA, Ames CP et al (2014) Total hospital costs of surgical treatment for adult spinal deformity: an extended follow-up study. Spine J 14:2326–2333
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
PDT and SD declare nothing to disclose, SWH lectures for Depuy-Synthes without financial renumeration.
Rights and permissions
About this article

Cite this article
Trobisch, P.D., Hwang, S.W. & Drange, S. PSO without neuromonitoring: analysis of peri-op complication rate after lumbar pedicle subtraction osteotomy in adults. Eur Spine J 25, 2629–2632 (2016). https://doi.org/10.1007/s00586-015-4278-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-4278-2