
Abstract
Purpose
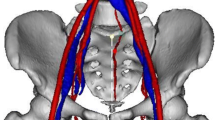
Pelvic and sacral surgeries are considered technically difficult due to the complex multidimensional anatomy and the presence of significant neurovascular structures. Knowledge of the key neurovascular anatomy is essential for safe and effective execution of partial and complete sacral resections. The goal of this anatomic, cadaveric study is to describe the pertinent neurovascular anatomy during these procedures.
Methods
Three embalmed human cadaveric specimens were used. Sacrectomies and sacroiliac joint resections were simulated and the structures at risk were identified. Both anterior and posterior approaches were evaluated.
Results
During sacroiliac joint resection, L5 nerve roots are at high risk for iatrogenic injury; the vasculatures at greatest risk are the common iliac vessels and internal iliac vessels with L5–S1 and S1–S2 high sacrectomies. Minor bleeding risk is associated with S2–S3 osteotomy because of the potential to damage superior gluteal vessels. S3–S4 osteotomy presents a low risk of bleeding. Adjacent nerve roots proximal to the resection level are at high risk during higher sacrectomies.
Conclusions
Several sacrectomy techniques are available and selection often depends on the specific case and surgeon preference; nevertheless, anatomic knowledge is extremely important. Considering the highly variable anatomic relations of the vascular bundles, a preoperative evaluation with CT or MRI with vascular reconstruction may be helpful to decrease bleeding risk by preemptively binding the internal iliac vessels in cases where higher tumors are present. To decrease the risk of damaging nerve roots, it is recommended to perform the resection as close to the involved foramina as possible.




Similar content being viewed by others


References
Unni KK, Inwards CY (2010) Dahlin’s Bone Tumors. Lippincott Williams & Wilkins, Philadelphia
Bergh P, Gunterberg B, Meis-Kindblom JM et al (2001) Prognostic factors and outcome of pelvic, sacral, and spinal chondrosarcomas: a center-based study of 69 cases. Cancer 91(7):1201–1212
Vaccaro AR, Kepler CK, Rihn JA et al (2012) Anatomical relationships of the anterior blood vessels to the lower lumbar intervertebral discs: analysis based on magnetic resonance imaging of patients in the prone position. J Bone Joint Surg Am 94(12):1088–1094
Pirró N, Ciampi D, Champsaur P et al (2005) The anatomical relationship of the iliocava junction to the lumbosacral spine and the aortic bifurcation. Surg Radiol Anat 27(2):137–141
Capellades J, Pellisé F, Rovira A et al (2000) Magnetic resonance anatomic study of iliocava junction and left iliac vein positions related to L5–S1 disc. Spine 25(13):1695–1700
Fătu C, Puişoru M, Fătu IC (2006) Morphometry of the internal iliac artery in different ethnic groups. Ann Anat 188(6):541–546
Sañudo JR, Mirapeix R, Rodriguez-Niedenführ M et al (2011) Obturator artery revisited. Int Urogynecol J 22(10):1313–1318
Pathi SD, Castellanos ME, Corton MM (2009) Variability of the retropubic space anatomy in female cadavers. Am J Obstet Gynecol 201(5):524.e1–524.e5
Holub Z, Lukac J, Kliment L et al (2005) Variability of the origin of the uterine artery: laparoscopic surgical observation. J Obstet Gynaecol Res 31(2):158–163
Zoccali C, Zoccali G, Bakaloudis G et al (2013) A new technique to perform pelvic osteotomy using Gigli saw. J Surg Oncol 108(2):136
Brunori A, Bruni P, Greco R et al (1995) Celebrating the centennial (1894–1994): Leonardo Gigli and his wire saw. J Neurosurg 82(6):1086–1090
Clarke MJ, Dasenbrock H, Bydon A et al (2012) Posterior-only approach for en bloc sacrectomy: clinical outcomes in 36 consecutive patients. Neurosurgery 71(2):357–364
Zhang HY, Thongtrangan I, Balabhadra RS et al (2003) Surgical techniques for total sacrectomy and spinopelvic reconstruction. Neurosurg Focus 15(2):E5
Gokaslan ZL, Romsdahl MM, Kroll SS et al (1997) Total sacrectomy and Galveston L-rod reconstruction for malignant neoplasms. Technical note. J Neurosurg 87(5):781–787
Fourney DR, Rhines LD, Hentschel SJ et al (2005) En bloc resection of primary sacral tumors: classification of surgical approaches and outcome. J Neurosurg Spine 3(2):111–122
Clarke MJ, Dasenbrock H, Bydon A et al (2012) Posterior-only approach for en bloc sacrectomy: clinical outcomes in 36 consecutive patients. Neurosurgery 71(2):357–364
Conflict of interest
The authors declare the absence of any conflict of interest or financial relationships pertaining to this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zoccali, C., Skoch, J., Patel, A. et al. The surgical neurovascular anatomy relating to partial and complete sacral and sacroiliac resections: a cadaveric, anatomic study. Eur Spine J 24, 1109–1113 (2015). https://doi.org/10.1007/s00586-015-3815-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-3815-3