
Abstract
Purpose
Recent studies suggest that the location of predominant pain (back or leg) can be a significant predictor of the outcome of surgery for degenerative spinal disorders. However, others challenge the notion that the predominant symptom can be reliably identified. This study examined the validity of a single item used to determine the most troublesome symptom.
Methods
A total of 2,778 patients with degenerative disorders of the lumbar spine scheduled for surgery with the goal of pain relief completed a questionnaire enquiring as to their most troublesome symptom [“main symptom”; back pain (BACK) or leg/buttock pain (LEG)]. They also completed separate 0–10 graphic rating scales for back pain (LBP) and leg/buttock pain (LP) intensity. Receiver operating characteristics (ROC) analysis was used to determine the accuracy with which the “LP minus LBP” score was able to classify patients into their declared “main symptom” group. Sub-studies evaluated the test–retest reliability of the patients’ self-rated pain scores (N = 45) and the agreement between the main symptom declared by the patient in the questionnaire and that documented by the surgeon after the clinical consultation (N = 118).
Results
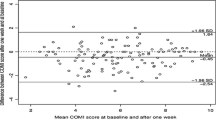
Test–retest reliability of the back and leg pain scores was good (ICC2,1 of 0.8 for each), as was patient–surgeon agreement regarding the main symptom (BACK or LEG) (κ value 0.79). In the BACK group, the mean values for pain intensity were 7.3 ± 2.0 (LBP) and 5.2 ± 2.9 (LP); in the LEG group, they were 4.3 ± 2.9 (LBP) and 7.5 ± 1.9 (LP). The area under the curve for the ROC was 0.95 (95 % CI 0.94–0.95), indicating excellent discrimination between the BACK and LEG groups based on the “LP minus LBP” scores. A cutoff score >0.0 for “LP minus LBP” score gave optimal sensitivity and specificity for indicating membership of the LEG group (sensitivity 79.1 %, specificity 95.7 %).
Conclusions
The responses on the single item for the “main symptom” were in good agreement with the differential ratings on the 0–10 pain scales for LBP and LP intensity. The cutoff >0 for “LP minus LBP” for classifying patients as LEG pain predominant seemed appropriate and suggests good concurrent validity for the single-item measure. The single item may be of use in sub-grouping patients with the same disorder (e.g. spondylolisthesis) or as an indication in surgical decision-making.


Similar content being viewed by others


References
Wai EK, Howse K, Pollock JW, Dornan H, Vexler L, Dagenais S (2009) The reliability of determining “leg dominant pain”. Spine J 9:447–453
Simon D, Coyle M, Dagenais S, O’Neil J, Wai EK (2009) Potential triaging of referrals for lumbar spinal surgery consultation: a comparison of referral accuracy from pain specialists, findings from advanced imaging and a 3-item questionnaire. Can J Surg 52:473–480
Postacchini F (1999) Surgical management of lumbar spinal stenosis. Spine 24:1043–1047
Atlas SJ, Keller RB, Robson D, Deyo RA, Singer DE (2000) Surgical and nonsurgical management of lumbar spinal stenosis: four-year outcomes from the maine lumbar spine study. Spine 25:556–562
Kleinstuck FS, Grob D, Lattig F, Bartanusz V, Porchet F, Jeszenszky D, O’Riordan D, Mannion AF (2009) The influence of preoperative back pain on the outcome of lumbar decompression surgery. Spine 34:1198–1203
Kleinstueck FS, Fekete T, Jeszenszky D, Mannion AF, Grob D, Lattig F, Mutter U, Porchet F (2011) The outcome of decompression surgery for lumbar herniated disc is influenced by the level of concomitant preoperative low back pain. Eur Spine J 20:1166–1173
Pearson A, Blood E, Lurie J, Abdu W, Sengupta D, Frymoyer JW, Weinstein J (2011) Predominant leg pain is associated with better surgical outcomes in degenerative spondylolisthesis and spinal stenosis: results from the Spine Patient Outcomes Research Trial (SPORT). Spine (Phila Pa 1976) 36:219–229
Kleinstueck FS, Fekete TF, Mannion AF, Grob D, Porchet F, Mutter U, Jeszenszky D (2012) To fuse or not to fuse in lumbar degenerative spondylolisthesis: do baseline symptoms help provide the answer? Eur Spine J 21:268–275
Zweig T, Mannion AF, Grob D, Melloh M, Munting E, Tuschel A, Aebi M, Roder C (2009) How to Tango: a manual for implementing Spine Tango. Eur Spine J 18(Suppl 3):312–320
Mannion AF, Elfering A, Staerkle R, Junge A, Grob D, Semmer NK, Jacobshagen N, Dvorak J, Boos N (2005) Outcome assessment in low back pain: how low can you go? Eur Spine J 14:1014–1026
Mannion AF, Porchet F, Kleinstück F, Lattig F, Jeszenszky D, Bartanusz V, Dvorak J, Grob D (2009) The quality of spine surgery from the patient’s perspective: part 1. The Core Outcome Measures Index (COMI) in clinical practice. Eur Spine J 18:367–373
Deyo RA, Centor RM (1986) Assessing the responsiveness of functional scales to clinical change: an analogy to diagnostic test performance. J Chronic Dis 39:897–906
Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, Bouter LM, de Vet HC (2007) Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol 60:34–42
Hopkins WG (2000) Measures of Reliability in Sports Medicine and Science. Sports Med 30:1–15
Davies HT, Crombie IK, Macrae WA (1998) Where does it hurt? Describing the body locations of chronic pain. Eur J Pain 2:69–80
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mannion, A.F., Mutter, U.M., Fekete, T.F. et al. Validity of a single-item measure to assess leg or back pain as the predominant symptom in patients with degenerative disorders of the lumbar spine. Eur Spine J 23, 882–887 (2014). https://doi.org/10.1007/s00586-014-3193-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3193-2