
Abstract
Purpose
Anterior cervical disectomy and fusion (ACDF) is a highly effective and safe method for spinal cord and cervical root decompression. However, vocal cord paralysis (VCP) remains an important cause of postoperative morbidity. The true incidence and recovery course of postoperative VCP is still uncertain. This study is a report on VCP after ACDF to evaluate the incidence, recovery course, and possible risk factors.
Methods
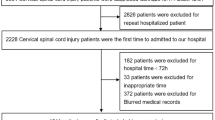
From 2004 to 2008, 1,895 consecutive patients underwent ACDF in our hospital and were followed up for at least 3 years. All surgeons were well trained and used a right-sided exposure. Prolonged VCP, where patients suffered from postoperative VCP lasting more than 3 months, was recorded and analyzed.
Results
In this retrospective study, 9 of the 1,895 patients (0.47 %) documented prolonged VCP lasting over 3 months. Six of the nine patients had total recovery within 9 months. Only three patients (0.16 %) still had symptoms even after 3 years postoperatively. All symptoms of VCP, except hoarseness, could be improved. After matching with 36 non-VCP patients, no differences with regard to longer operative or anesthesia time, shorter neck, obesity, and prevertebral edema. All cases of prolonged course of postoperative VCP occurred in patients who underwent exposure at the C67 level.
Conclusion
In our study, only 0.47 % documented prolonged postoperative VCP, while most patients recovered within 9 months. However, if symptoms last longer, there could be almost permanent VCP (0.16 %). In our study, choking and dysphagia subsided mostly within 6 months, but hoarseness remained. The exposure of the C67 level obviously was a risk factor for postoperative VCP.
Similar content being viewed by others


References
Kriskovich MD, Apfelbaum RI, Haller JR (2000) Vocal fold paralysis after anterior cervical spine surgery: incidence, mechanism, and prevention of injury. Laryngoscope 110:1467–1473. doi:10.1097/00005537-200009000-00011
Apfelbaum RI, Kriskovich MD, Haller JR (2000) On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine 25:2906–2912
Audu P, Artz G, Scheid S, Harrop J, Albert T, Vaccaro A, Hilibrand A, Sharan A, Spiegal J, Rosen M (2006) Recurrent laryngeal nerve palsy after anterior cervical spine surgery: the impact of endotracheal tube cuff deflation, reinflation, and pressure adjustment. Anesthesiology 105:898–901
Beutler WJ, Sweeney CA, Connolly PJ (2001) Recurrent laryngeal nerve injury with anterior cervical spine surgery risk with laterality of surgical approach. Spine 26:1337–1342
Kilburg C, Sullivan HG, Mathiason MA (2006) Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 4:273–277. doi:10.3171/spi.2006.4.4.273
Dimopoulos VG, Chung I, Lee GP, Johnston KW, Kapsalakis IZ, Smisson HF 3rd, Grigorian AA, Robinson JS Jr, Fountas KN (2009) Quantitative estimation of the recurrent laryngeal nerve irritation by employing spontaneous intraoperative electromyographic monitoring during anterior cervical discectomy and fusion. J Spinal Disord Tech 22:1–7. doi:10.1097/BSD.0b013e31815ea8b6
Morpeth JF, Williams MF (2000) Vocal fold paralysis after anterior cervical diskectomy and fusion. The Laryngoscope 110:43–46. doi:10.1097/00005537-200001000-00009
Jung A, Schramm J (2010) How to reduce recurrent laryngeal nerve palsy in anterior cervical spine surgery: a prospective observational study. Neurosurgery 67:10–15. doi:10.1227/01.NEU.0000370203.26164.24 discussion 15
Jung A, Schramm J, Lehnerdt K, Herberhold C (2005) Recurrent laryngeal nerve palsy during anterior cervical spine surgery: a prospective study. J Neurosurg Spine 2:123–127. doi:10.3171/spi.2005.2.2.0123
Zeidman SM, Ducker TB, Raycroft J (1997) Trends and complications in cervical spine surgery: 1989–1993. J Spinal Disord 10:523–526
Netterville JL, Koriwchak MJ, Winkle M, Courey MS, Ossoff RH (1996) Vocal fold paralysis following the anterior approach to the cervical spine. Ann Otol Rhinol Laryngol 105:85–91
Heeneman H (1973) Vocal cord paralysis following approaches to the anterior cervical spine. Laryngoscope 83:17–21. doi:10.1288/00005537-197301000-00002
Postma GN, Shockley WW (1998) Transient vocal fold immobility. Ann Otol Rhinol Laryngol 107:236–240
Tew JM Jr, Mayfield FH (1976) Complications of surgery of the anterior cervical spine. Clin Neurosurg 23:424–434
Terris DJ, Arnstein DP, Nguyen HH (1992) Contemporary evaluation of unilateral vocal cord paralysis. Otolaryngol Head Neck Surg 107:84–90
Benninger MS, Gillen JB, Altman JS (1998) Changing etiology of vocal fold immobility. Laryngoscope 108:1346–1350
Jellish WS, Jensen RL, Anderson DE, Shea JF (1999) Intraoperative electromyographic assessment of recurrent laryngeal nerve stress and pharyngeal injury during anterior cervical spine surgery with Caspar instrumentation. J Neurosurg 91:170–174
Sperry RJ, Johnson JO, Apfelbaum RI (1993) Endotracheal tube cuff pressure increases significantly during anterior cervical fusion with the Caspar instrumentation system. Anesth Analg 76:1318–1321
Weisberg NK, Spengler DM, Netterville JL (1997) Stretch-induced nerve injury as a cause of paralysis secondary to the anterior cervical approach. Otolaryngol Head Neck Surg 116:317–326
Razfar A, Sadr-Hosseini SM, Rosen CA, Snyderman CH, Gooding W, Abla AA, Ferris RL (2012) Prevention and management of dysphonia during anterior cervical spine surgery. Laryngoscope 122:2179–2183. doi:10.1002/lary.23284
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, CC., Huang, YC., Lee, ST. et al. Long-term result of vocal cord paralysis after anterior cervical disectomy. Eur Spine J 23, 622–626 (2014). https://doi.org/10.1007/s00586-013-3084-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-013-3084-y