
Abstract
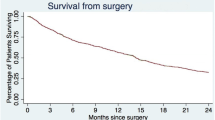
We present survival, neurological function, and complications in a consecutive series of 282 patients operated for spinal metastases from January 1990 to December 2001. Our main surgical indication throughout this time period was neurological deficit rather than pain. Metastases from cancer of the prostate accounted for 40%, breast 15%, kidney 8%, and lung 7%. In 78% the level of decompression was thoracic and lumbar in 22%. Thirteen percent had a single metastases only, 64% had multiple skeletal metastases, and 23% had non-skeletal metastases also. Preoperatively 64% were non-walkers (Frankel A-C), 30% could walk with aids (Frankel D) and 8% had normal motor function (Frankel E). Posterior decompression and stabilization was applied in 212 patients, 47 had laminectomy only, and 23 had anterior decompressions and reconstruction. Complications were recorded at a level of 20%, and systemic complications were often associated with early death. The survival rate was 0.63 at 3 months, 0.47 at 6 months, 0.30 at 1 year, and 0.16 at 2 years. Twelve of 255 (5%) patients with motor deficits were worsened postoperatively, whereas 179 (70%) improved at least one Frankel grade. The ability to walk postoperatively was retained during follow-up in more than 80% of the patients. This study shows that important improvement of function can be gained by surgical treatment, but the complication rate was high and many patients died of their disease within the first months of surgery.


Similar content being viewed by others


References
Aebi M (2003) Spinal metastasis in the elderly. Eur Spine J 12 (Suppl 2):S202–S213
Bauer HC (1997) Posterior decompression and stabilization for spinal metastases: analysis of sixty-seven consecutive patients. J Bone Joint Surg Am 79:514–522
Bauer HCF, Wedin R (1995) Survival after surgery for spinal and extremity metastases: prognostication in 241 patients. Acta Orthop Scand 66:143–146
Bone Pain Trial Working Party (1999) 8 Gy single fraction radiotherapy for the treatment of metastatic skeletal pain: randomised comparison with a multifraction schedule over 12 months of patient follow-up. Radiother Oncol 52:111–121
Clayton D, Hills M (1993) Statistical models in epidemiology. Oxford University Press, Oxford
Davis LA, Warren SA, Reid DC, Oberle K, Saboe LA, Grace MAG (1993) Incomplete neural deficits in thoracolumbar and lumbar spine fractures. Spine 18:257–263
Finkelstein JA, Zaveri G, Wai E, Vidmar M, Kreder H, Chow E (2003) A population-based study of surgery for spinal metastases. J Bone Joint Surg Br 85:1045–1050
Frankel HL, Hancock DO, Hyslop G et al (1969) The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. Paraplegia 7:179–192
Harrington KD (1988) Anterior decompression and stabilization of the spine as treatment for vertebral collapse and spinal cord compression from metastatic malignancy. Clin Orthop 227:103–112
Lee CK, Rosa R, Fernand R (1986) Surgical treatment of tumors of the spine. Spine 11:201–208
Loblaw AD, Laperriere NJ (1998) Emergency treatment of malignant extradural spinal cord compression: An evidence-based guideline. J Clin Oncol 16:1613–1624
Obermair A, Handisurya A, Kaider A, Sevelda P, Kolbl H, Gitsch G (1998) The relationship of pretreatment serum hemoglobin level to the survival of epithelial ovarian carcinoma patients: a prospective review. Cancer 83:726–731
Pointillart, Ravaud A, Palussière J (2002) Vertebral metastases. Springer, Berlin Heiddberg New York
Regine WF, Tibbs PA, Young A, Payne R, Saris S, Kryscio RJ et al. (2003) Metastatic spinal cord compression: a randomized trial of direct decompressive surgical resection plus radiotherapy vs. radiotherapy alone. Int J Radiat Oncol Biol Phys 57(Suppl 2):125
Rompe JD, Hopf CG, Eysel P (1999) Outcome after palliative posterior surgery for metastatic disease of the spine-evaluation of 106 consecutive patients after decompression and stabilization with the Cotrel-Dubousset instrumentation. Arch Orthop Trauma Surg 119:394–400
Steenland E, Leer J, van Houwelingen H, Post WJ, van den Hout WB, Kievit et al (1999) The effect of a single fraction compared to multiple fractions on painful bone metastases: a global analyses of the Dutch Bone Metastasis Study. Radiotherapy Oncol 52:101–109
Sundaresan N, Rothman A, Manhart K, Kelliher (2002) Surgery for solitary metastases of the spine: rationale and results of treatment. Spine 27:1802–1806
Sundaresan N, Sachdev VP, Holland JF, Moore F, Sung M, Paciucci PA et al (1995) Surgical treatment of spinal cord compression from epidural metastasis. J Clin Oncol 13:2330–2335
Tokuhashi Y, Matsuzaki H, Toriyama S, Kawano H, Ohssaka S (1990) Scoring system for preoperative evaluation or metastatic spine tumor prognosis. Spine 15:1110–1113
Tomita K, Kawahara N, Kobayashi T, Yoshida A, Murakami H, Akamaru T (2001) Surgical strategy for spinal metastases. Spine 26:298–306
Wedin R, Bauer HFC, Skoog L, Söderlund V, Tani E (2000) Cytological diagnosis of skeletal lesions. Fine-needle aspiration biopsy in 110 tumours. J Bone Joint Surg Br 82:673–678
Wenger M (2003) Vertebroplasty for metastasis. Med Oncol 20:203–209
Wise JJ, Fishgrund JS, Herkowitz HN, Montgomery D, Kurz LT (1999) Complication, survival rates, and risk factors of surgery for metastatic disease of the spine. Spine 24:1943–1951
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jansson, KÅ., Bauer, H.C.F. Survival, complications and outcome in 282 patients operated for neurological deficit due to thoracic or lumbar spinal metastases. Eur Spine J 15, 196–202 (2006). https://doi.org/10.1007/s00586-004-0870-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-004-0870-6