
Abstract
Purpose
Robotic prostatectomy is the most common surgical approach for treating prostate cancer. Patients undergoing robotic prostatectomy may have bullae, which may rupture leading to pneumothorax. We evaluated the incidence of pneumothorax due to preoperative bullae rupture in robotic prostatectomy.
Methods
A large retrospective study of patients who underwent robotic prostatectomy between 2009 and 2021 was conducted. Bullae were detected using chest computed tomography. Pneumothorax was detected using a chest X-ray. The primary outcome was the incidence of pneumothorax due to bullae rupture. Secondary outcomes were the prevalence of preoperative bullae and the evaluation of postoperative outcomes, including length of hospital stay, intensive care unit admission rate, and prolonged intensive care unit stay (> 2 days).
Results
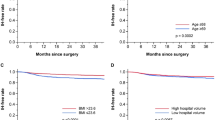
A total of 6605 patients were included. The prevalence of preoperative bullae was 3.0% (196/6,605). There was no incidence of pneumothorax due to bullae rupture. No significant difference in the incidences of pneumothorax between patients with and without bullae (0/196 vs. 2/6,409, P > 0.999) was observed. In addition, length of hospital stay, intensive care unit admission rate, and prolonged intensive care unit stay were not significantly different between the two groups. Kaplan–Meier analysis showed that there was no significant difference in lengths of hospital stay between the two groups (log-rank test, P > 0.999).
Conclusion
In our cohort, there was no incidence of pneumothorax following robotic prostatectomy in patients with preoperative bullae. This result could help in the management of patients with prostate cancer with bullae.

Similar content being viewed by others


References
Ogilvie C, Catterall M. Patterns of disturbed lung function in patients with emphysematous bullae. Thorax. 1959;14:216–24.
Saini V, Assu SM, Bhatia N, Sethi S. Abdominal surgery in a patient with bullous emphysema: anesthetic concerns. J Anaesthesiol Clin Pharmacol. 2019;35:414–5.
Bansal S, Surve RM, Venkatapura RJ. Anesthetic management of a paraparetic patient with multiple lung bullae. J Neurosurg Anesthesiol. 2014;26:85–6.
Binder J, Kramer W. Robotically-assisted laparoscopic radical prostatectomy. BJU Int. 2001;87:408–10.
Trinh QD, Sammon J, Sun M, Ravi P, Ghani KR, Bianchi M, Jeong W, Shariat SF, Hansen J, Schmitges J, Jeldres C, Rogers CG, Peabody JO, Montorsi F, Menon M, Karakiewicz PI. Perioperative outcomes of robot-assisted radical prostatectomy compared with open radical prostatectomy: results from the nationwide inpatient sample. Eur Urol. 2012;61:679–85.
Tsui C, Klein R, Garabrant M. Minimally invasive surgery: national trends in adoption and future directions for hospital strategy. Surg Endosc. 2013;27:2253–7.
Danic MJ, Chow M, Alexander G, Bhandari A, Menon M, Brown M. Anesthesia considerations for robotic-assisted laparoscopic prostatectomy: a review of 1500 cases. J Robot Surg. 2007;1:119–23.
Kalmar AF, Foubert L, Hendrickx JF, Mottrie A, Absalom A, Mortier EP, Struys MM. Influence of steep Trendelenburg position and CO2 pneumoperitoneum on cardiovascular, cerebrovascular, and respiratory homeostasis during robotic prostatectomy. Br J Anaesth. 2010;104:433–9.
Yu J, Park JY, Kim DH, Kim S, Hwang JH, Seo H, Kim YK. Incidence and risk factors of pulmonary complications after robot-assisted laparoscopic prostatectomy: a retrospective observational analysis of 2208 patients at a large single center. J Clin Med. 2019;8:1509.
Yu J, Park JY, Hong JH, Hwang JH, Kim YK. Effect of pneumoperitoneum and Trendelenburg position on internal carotid artery blood flow measured by ultrasound during robotic prostatectomy. Clin Physiol Funct Imaging. 2022;42:139–45.
Gainsburg DM. Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy. Minerva Anestesiol. 2012;78:596–604.
Zompatori M, Fasano L, Battista G, Canini R. Diagnostic imaging of bullous pulmonary disease. A review. Radiol Med. 1998;96:161–7.
Teramoto S, Fukuchi Y, Nagase T, Matsuse T, Shindo G, Orimo H. Quantitative assessment of dyspnea during exercise before and after bullectomy for giant bulla. Chest. 1992;102:1362–6.
Schipper PH, Meyers BF, Battafarano RJ, Guthrie TJ, Patterson GA, Cooper JD. Outcomes after resection of giant emphysematous bullae. Ann Thorac Surg. 2004;78:976–82.
Sharma KC, Brandstetter RD, Brensilver JM, Jung LD. Cardiopulmonary physiology and pathophysiology as a consequence of laparoscopic surgery. Chest. 1996;110:810–5.
Brister NW, Barnette RE, Kim V, Keresztury M. Anesthetic considerations in candidates for lung volume reduction surgery. Proc Am Thorac Soc. 2008;5:432–7.
Bense L, Lewander R, Eklund G, Hedenstierna G, Wiman LG. Nonsmoking, non-alpha 1-antitrypsin deficiency-induced emphysema in nonsmokers with healed spontaneous pneumothorax, identified by computed tomography of the lungs. Chest. 1993;103:433–8.
Lesur O, Delorme N, Fromaget JM, Bernadac P, Polu JM. Computed tomography in the etiologic assessment of idiopathic spontaneous pneumothorax. Chest. 1990;98:341–7.
Amjadi K, Alvarez GG, Vanderhelst E, Velkeniers B, Lam M, Noppen M. The prevalence of blebs or bullae among young healthy adults: a thoracoscopic investigation. Chest. 2007;132:1140–5.
Bang DH, Lim D, Jeong OM, Hwang WS, Jung JY, Lim J. Low-dose chest computed tomography as a screening tool: findings in 536 aircrews. Aviat Space Environ Med. 2012;83:896–8.
Park HJ, Kim DK, Yang MK, Seo JE, Kwon JH. Carbon dioxide pneumothorax occurring during laparoscopy-assisted gastrectomy due to a congenital diaphragmatic defect: a case report. Korean J Anesthesiol. 2016;69:88–92.
Karayiannakis AJ, Anagnostoulis S, Michailidis K, Vogiatzaki T, Polychronidis A, Simopoulos C. Spontaneous resolution of massive right-sided pneumothorax occurring during laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2005;15:100–3.
Wahba RW, Tessler MJ, Kleiman SJ. Acute ventilatory complications during laparoscopic upper abdominal surgery. Can J Anaesth. 1996;43:77–83.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.

540_2022_3111_MOESM1_ESM.jpg
Supplementary file1 Comparison of the incidences of pneumothorax between patients with and without bullae. Note that there is no significant difference in the incidences of pneumothorax between patients with and without bullae (JPG 1386 KB)

540_2022_3111_MOESM2_ESM.jpg
Supplementary file2 Kaplan–Meier analysis for lengths of hospital stay between patients with and without bullae. Note that there is no significant difference in the lengths of hospital stay between patients with and without bullae (JPG 2709 KB)
About this article

{kind=link}
{kind=link}
Cite this article
Yu, J., Park, JY., Lee, J. et al. Preoperative bullae and subsequent pneumothorax in 6605 patients who underwent robotic prostatectomy. J Anesth 36, 740–746 (2022). https://doi.org/10.1007/s00540-022-03111-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-022-03111-1