
Abstract
Purpose
The aim of this study was to assess the efficacy of programmed intermittent epidural boluses (PIEB) in postoperative pain management compared with continuous epidural infusion (CEI) after cesarean delivery.
Methods
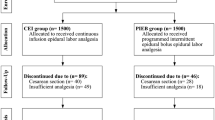
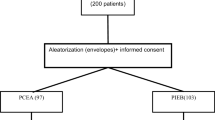
A total of 58 participants were randomly allocated to receive PIEB (3 mL bolus every 60 min) or CEI (3 mL/h) for postoperative analgesia after undergoing elective cesarean section under combined spinal–epidural anesthesia. Both groups had the same epidural solution containing ropivacaine 0.2% plus fentanyl 2 µg/mL. The primary outcome was postoperative pain score at rest and mobilization at 6, 12, 24, and 48 h. The secondary outcomes were the total amount of ropivacaine used in the 48 h study period and the time to the first PCEA bolus.
Results
Data from 58 women were analyzed. There was a reduction in pain verbal numerical rating scores at 12 h in patients receiving PIEB compared with CEI at rest [2 (1.75–3) vs. 3 (2–4), p = 0.011]; and on movement [4 (3–5) vs. 5 (4–6), p = 0.038]. No differences were found in pain scores at any other time-point up to 48 h. Total ropivacaine consumption at 48 h was less in the PIEB group compared with the CEI group [316 mg (304–321) vs. 336 mg (319–344), p = 0.001].
Conclusion
Postoperative epidural analgesia for patients who underwent cesarean delivery with PIEB compared with CEI resulted in less ropivacaine usage while providing comparable analgesia.




Similar content being viewed by others

References
Leung AY. Postoperative pain management in obstetric anesthesia—new challenges and solutions. J Clin Anesth. 2004;16(1):57–65.
Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA Jr, Wu CL. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA. 2003;290(18):2455–63.
Chua SM, Sia AT. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labour. Can J Anaesth. 2004;51(6):581–5.
Wong CA, Ratliff JT, Sullivan JT, Scavone BM, Toledo P, McCarthy RJ. A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia. Anesth Analg. 2006;102(3):904–9.
Capogna G, Camorcia M, Stirparo S, Farcomeni A. Programmed intermittent epidural bolus versus continuous epidural infusion for labor analgesia: the effects on maternal motor function and labor outcome. A randomized double-blind study in nulliparous women. Anesth Analg. 2011;113(4):826–31.
Wong CA, McCarthy RJ, Hewlett B. The effect of manipulation of the programmed intermittent bolus time interval and injection volume on total drug use for labor epidural analgesia: a randomized controlled trial. Anesth Analg. 2011;112(4):904–11.
George RB, Allen TK, Habib AS. Intermittent epidural bolus compared with continuous epidural infusions for labor analgesia: a systematic review and meta-analysis. Anesth Analg. 2013;116(1):133–44.
Carvalho B, George RB, Cobb B, McKenzie C, Riley ET. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123(4):965–71.
Breen TW, Shapiro T, Glass B, Foster-Payne D, Oriol NE. Epidural anesthesia for labor in an ambulatory patient. Anesth Analg. 1993;77(5):919–24.
Fettes PD, Moore CS, Whiteside JB, McLeod GA, Wildsmith JA. Intermittent vs continuous administration of epidural ropivacaine with fentanyl for analgesia during labour. Br J Anaesth. 2006;97(3):359–64.
Hogan Q. Distribution of solution in the epidural space: examination by cryomicrotome section. Reg Anesth Pain Med. 2002;27(2):150–6.
Xu J, Zhou J, Xiao H, Pan S, Liu J, Shang Y, Yao S. A systematic review and meta-analysis comparing programmed intermittent bolus and continuous infusion as the background infusion for parturient-controlled epidural analgesia. Sci Rep. 2019;9(1):2583.
Satomi S, Kakuta N, Murakami C, Sakai Y, Tanaka K, Tsutsumi YM. The efficacy of programmed intermittent epidural bolus for postoperative analgesia after open gynecological surgery: a randomized double-blinded study. Biomed Res Int. 2018;2018:6297247.
Wiesmann T, Hoff L, Prien L, Torossian A, Eberhart L, Wulf H, Feldmann C. Programmed intermittent epidural bolus versus continuous epidural infusion for postoperative analgesia after major abdominal and gynecological cancer surgery: a randomized, triple-blinded clinical trial. BMC Anesthesiol. 2018;18(1):154.
Myles PS, Myles DB, Galagher W, Boyd D, Chew C, MacDonald N, Dennis A. Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth. 2017;118(3):424–9.
Kaynar AM, Shankar KB. Epidural infusion: continuous or bolus? Anesth Analg. 1999;89(2):534.
Ojo OA, Mehdiratta JE, Gamez BH, Hunting J, Habib AS. Comparison of programmed intermittent epidural boluses with continuous epidural infusion for the maintenance of labor analgesia: a randomized, controlled. Double-Blind Study Anesth Analg. 2020;130(2):426–35.
Epsztein Kanczuk M, Barrett NM, Arzola C, Downey K, Ye XY, Carvalho JC. Programmed intermittent epidural bolus for labor analgesia during first stage of labor: a biased-coin up-and-down sequential allocation trial to determine the optimum interval time between boluses of a fixed volume of 10 mL of bupivacaine 0.0625% with fentanyl 2 mug/mL. Anesth Analg. 2017;124(2):537–41.
Zakus P, Arzola C, Bittencourt R, Downey K, Ye XY, Carvalho JC. Determination of the optimal programmed intermittent epidural bolus volume of bupivacaine 0.0625% with fentanyl 2 mug.ml (−1) at a fixed interval of forty minutes: a biased coin up-and-down sequential allocation trial. Anaesthesia. 2018;73(4):459–65.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Wang, L., Wu, Z., Hu, L. et al. Programmed intermittent epidural bolus for post-cesarean delivery analgesia: a randomized controlled double-blind trial. J Anesth 36, 32–37 (2022). https://doi.org/10.1007/s00540-021-03002-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-021-03002-x