
Abstract
Purpose
An endoscopic bite block is a device to ensure that the patient’s mouth remains wide open during endoscopic procedures. Wide opening of the mouth may facilitate the efficiency of one-handed mask ventilation. We evaluated the effect of an endoscopic bite block on mask ventilation among three ventilation techniques: one-handed ventilation, one-handed ventilation with an endoscopic bite block, and two-handed ventilation.
Methods
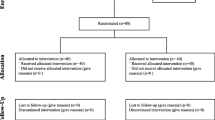
Fifty-nine anesthetized and paralyzed patients were included. After induction of anesthesia, one-handed ventilation, one-handed ventilation with an endoscopic bite block and two-handed ventilation were performed in a cross-over, randomized order. The primary outcome was the expiratory tidal volume (mL/kg of predicted body weight). Secondary outcomes included minute ventilation (L/min) and the incidence of inadequate mask ventilation or dead space ventilation.
Results
The expiratory tidal volume of one-handed ventilation with an endoscopic bite block was significantly improved when compared with that of one-handed ventilation (8.2 [6.8–10.2] mL/kg vs. 7.1 [4.5–9.0] mL/kg, respectively, difference = 1.1 mL/kg; 95% CI 0.8–2.4; P < 0.001), and was comparable to that of two-handed ventilation (8.9 [6.3–11.5] mL/kg; difference = 0.7 mL/kg; 95% CI − 0.7 to 1.5; P = 0.432). Minute ventilation was also significantly improved in one-handed ventilation with an endoscopic bite block compared with that in one-handed ventilation (7.4 [6.3–8.6] L/min vs. 6.7 [4.2–7.9] L/min, respectively, difference = 0.7 L/min; 95% CI 0.6–2.0; P < 0.001), and was comparable to that of two-handed ventilation (7.7 [6.5–9.5] L/min; difference = 0.3 L/min; 95% CI − 0.5 to 1.4; P = 0.390). The incidence of inadequate ventilation or dead space ventilation was not different among the ventilation techniques (P = 0.080).
Conclusion
The use of an endoscopic bite block improved one-handed mask ventilation, showing comparable efficacy with two-handed mask ventilation.

Similar content being viewed by others


References
Safar P, Escarraga LA, Elam JO. A comparison of the mouth-to-mouth and mouth-to-airway methods of artificial respiration with the chest-pressure arm-lift methods. N Engl J Med. 1958;258:671–7.
Kheterpal S, Han R, Tremper KK, Shanks A, Tait AR, O'Reilly M, Ludwig TA. Incidence and predictors of difficult and impossible mask ventilation. Anesthesiology. 2006;105:885–91.
Kheterpal S, Martin L, Shanks AM, Tremper KK. Prediction and outcomes of impossible mask ventilation: a review of 50,000 anesthetics. Anesthesiology. 2009;110:891–7.
Joffe AM, Hetzel S, Liew EC. A two-handed jaw-thrust technique is superior to the one-handed "EC-clamp" technique for mask ventilation in the apneic unconscious person. Anesthesiology. 2010;113:873–9.
Hart D, Reardon R, Ward C, Miner J. Face mask ventilation: a comparison of three techniques. J Emerg Med. 2013;44:1028–33.
Hagberg CA. Benumof and Hagberg's Airway management. 3rd ed. Philadelphia: Elsevier; 2013.
Isono S. One hand, two hands, or no hands for maximizing airway maneuvers? Anesthesiology. 2008;109:576–7.
Wilson ME, Spiegelhalter D, Robertson JA, Lesser P. Predicting difficult intubation. Br J Anaesth. 1988;61:211–6.
Han R, Tremper KK, Kheterpal S, O'Reilly M. Grading scale for mask ventilation. Anesthesiology. 2004;101:267.
Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A, Acure Respiratory Distress Syndrome N. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New Engl J Med. 2000;342:1301–8.
Langeron O, Masso E, Huraux C, Guggiari M, Bianchi A, Coriat P, Riou B. Prediction of difficult mask ventilation. Anesthesiology. 2000;92:1229–366.
Bachiller PR, McDonough JM, Feldman JM. Do new anesthesia ventilators deliver small tidal volumes accurately during volume-controlled ventilation? Anesth Analg. 2008;106:1392–400.
Glenski TA, Diehl C, Clopton RG, Friesen RH. Breathing circuit compliance and accuracy of displayed tidal volume during pressure-controlled ventilation of infants: a quality improvement project. Pediatr Anaesth. 2017;27:935–41.
Warters RD, Szabo TA, Spinale FG, DeSantis SM, Reves JG. The effect of neuromuscular blockade on mask ventilation. Anaesthesia. 2011;66:163–7.
Ikeda A, Isono S, Sato Y, Yogo H, Sato J, Ishikawa T, Nishino T. Effects of muscle relaxants on mask ventilation in anesthetized persons with normal upper airway anatomy. Anesthesiology. 2012;117:487–93.
Isono S, Tanaka A, Tagaito Y, Sho Y, Nishino T. Pharyngeal patency in response to advancement of the mandible in obese anesthetized persons. Anesthesiology. 1997;87:1055–62.
Acknowledgements
The authors would like to thank Sohee Oh, PhD of the Department of Biostatistics in Seoul Metropolitan Government Seoul National University Boramae Medical Center for statistical advice.
Funding
This study was not funded.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Kim, H., Chang, JE., Lee, JM. et al. Effect of an endoscopic bite block on one-handed mask ventilation. J Anesth 34, 211–216 (2020). https://doi.org/10.1007/s00540-019-02732-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-019-02732-3