
Abstract
Purpose
This prospective, observational study was performed to examine the hypothesis that if conventional 7-cm head elevation is applied, laryngoscopy is more difficult for patients with anteroposterior chest diameter (chest AP diameter) outside the average range (≥17.7 or ≤14.7 cm).
Methods
Chest AP diameter at the sternal notch were measured preoperatively. All patients were placed on a surgical bed with an incompressible 7-cm pillow. During laryngoscopy, the laryngeal view was graded by use of the Cormack–Lehane classification. Difficult visualization of the larynx (DVL) was defined as a grade 3 or 4 view.
Results
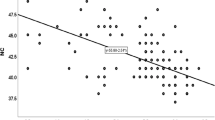
DVL was observed for 49 patients (18.2 %). Differences between measured chest AP diameter for each patient and the calculated median value were used for statistical analysis. In univariate analysis, the difference between chest AP diameter and the median value was significantly related to DVL. Logistic regression analysis confirmed that the difference between chest AP diameter and the median value was an independent predictor of DVL (odds ratio, 3.900; 95 % confidence interval, 2.371–6.415; p < 0.001). Receiver operating characteristic curve analysis showed that this test with a test threshold of 1.5 cm had reasonable diagnostic accuracy (area under the curve of 0.748).
Conclusion
When using a standard pillow size of 7 cm, chest AP diameter above or below the average range (≥17.7 or ≤14.7 cm) was a strong predictor of DVL for apparently normal-sized patients. In such cases, modification of pillow height should be considered.


Similar content being viewed by others


References
Adnet F, Baillard C, Borron SW, Denantes C, Lefebvre L, Galinski M, Martinez C, Cupa M, Lapostolle F. Randomized study comparing the “sniffing position” with simple head extension for laryngoscopic view in elective surgery patients. Anesthesiology. 2001;95:836–41.
El-Orbany M, Woehlck H, Salem MR. Head and neck position for direct laryngoscopy. Anesth Analg. 2011;113:03–9.
Benumof JL. Comparison of intubating positions: the end point of for position should be measured. Anesthesiology. 2002;97:750.
Schmitt HJ, Mang H. Head and neck elevation beyond the sniffing position improves laryngeal view in cases of difficult direct laryngoscopy. J Clin Anesth. 2002;14:335–8.
Collins JS, Lemmens HJ, Brodsky JB, Brock-Utne JG, Levitan RM. Laryngoscopy and morbid obesity: a comparison of the “sniff” and “ramped” positions. Obes Surg. 2004;14:1171–5.
Sivarajan M, Joy JV. Effect of general anesthesia and paralysis on upper airway changes due to head position. Anesthesiology. 1996;85:787–93.
Samsoon GL, Young JR. Difficult tracheal intubation: a retrospective study. Anaesthesia. 1987;42:487–90.
Savva D. Prediction of difficult tracheal intubation. Br J Anaesth. 1994;73:149–53.
Huh J, Shin HY, Kim SH, Yoon TK, Kim DK. Diagnostic predictor of difficult laryngoscopy: the hyomental distance ratio. Anesth Analg. 2009;108:544–8.
Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984;39:1105–11.
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the area under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44:837–45.
Greenland KB, Edward MJ, Hutton NJ, Challis VJ, Irwin MG, Sleigh JW. Changes in airway configuration with different head and neck positions using magnetic resonance imaging of normal airway: a new concept with possible clinical applications. Br J Anaesth. 2010;105:683–90.
Greenland KB, Edward MJ, Hutton NJ. External auditory meatus-sternal notch relationship in adults in the sniffing position: a magnetic resonance imaging study. Br J Anaesth. 2010;104:268–9.
Isono S. Common practice and concepts in anesthesia: time for reassessment: is the sniffing position a “gold standard” for laryngoscopy? Anesthesiology. 2001;95:825–7.
Kitamura Y, Isono S, Suzuki N, Sato Y, Nishino T. Dynamic interaction of craniofacial structures during head positioning and direct laryngoscopy in anesthetized patients with and without difficult laryngoscopy. Anesthesiology. 2007;107:875–83.
Lee A, Fan LT, Gin T, Karmakar MK, NganKee WD. A systemic review (meta-analysis) of the accuracy of the Mallampati tests to predict the difficult airway. Anesth Analg. 2006;102:1867–78.
Benumof JL. Management of the difficult adult airway. With special emphasis on awake tracheal intubation. Anesthesiology. 1991;75:1087–110.
Cook TM. A new practical classification of laryngeal view. Anaesthesia. 2000;55:274–9.
Horton WA, Fahy L, Charters P. Defining a standard intubating position using “angle finder”. Br J Anaesth. 1989;62:6–12.
Carlson MD, Morrison RS. Study design, precision, and validity in observational studies. J Palliat Med. 2009;12:77–82.
Naing L, Winn T, Rusli BN. Practical issues in calculating the sample size for prevalence studies. Arch Orofac Sci. 2006;1:9–14.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was registered with Clinical Research Information Service (CRIS; http://cris.cdc.go.kr/cris/en/use_guide/cris_introduce.jsp) (ref: KCT0000395).
About this article
Cite this article
Choi, JW., Kim, JA., Kim, HK. et al. Chest anteroposterior diameter affects difficulty of laryngoscopy for non-morbidly obese patients. J Anesth 27, 563–568 (2013). https://doi.org/10.1007/s00540-013-1572-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-013-1572-1