
Abstract
Purpose
Several studies have reported that sevoflurane was associated with a relatively high incidence of emergence agitation in children even in the absence of any surgical intervention. The aim of this study was to compare early agitation characteristics of oral melatonin, dexmedetomidine, and midazolam premedication in children who were given sevoflurane anesthesia for esophageal dilatation.
Methods
Following Internal Review Board approval and parental informed consent, 100 ASA physical status I–II children (3–9 years old) who were scheduled to undergo general anesthesia for esophageal dilatation procedures were enrolled. The patients were randomly assigned to four groups (n = 25 in each). The premedications in the groups were saline (group P), dexmedetomidine 2.5 μg/kg (group D), 0.5 mg/kg midazolam (group MD), and melatonin 0.1 mg/kg (group ML), given orally. All premedication drugs were given with paracetamol 2–2.5 mg/kg to be easily drinkable 40–45 min before anesthesia induction. Anesthesia was maintained with sevoflurane 2–4%, N2O 50% in oxygen. No supplemental analgesic agent was given, and an emergence agitation scale (EAS) was measured on admission to the PACU, then every 5 min, and recorded during the postoperative period: 1, awake and calm, cooperative; 2, crying, requires consoling; 3, irritable/restless, screaming, inconsolable; 4, combative, disoriented, thrashing. Children with an agitation score of 3 or 4 were classified as agitated.
Results
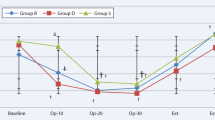
There were no significant differences among the four groups demographically. The emergence agitation scale was higher in the placebo group than in the others at 5, 10, and 15 min postoperatively (P < 0.001). EA was similar among group D, group MD, and group ML.
Conclusion
We found that oral melatonin, dexmedetomidine, and midazolam reduced the incidence of emergence agitation in children after sevoflurane anesthesia.
Similar content being viewed by others


References
Cravero J, Surgenor S, Whalen K. Emergence agitation in paediatric patients after sevoflurane anaesthesia and no surgery: a comparison with halothane. Paediatr Anaesth. 2000;10:419–24.
Beskow A, Westrin P. Sevoflurane causes more postoperative agitation in children than does halothane. Acta Anaesthsiol Scand. 1999;43:536–41.
Silva LM, Braz LG, Módolo NS. Emergence agitation in pediatric anesthesia: current features. J Pediatr. 2008;84:107–13.
Goa KL, Noble S, Spencer CM. Sevoflurane in paediatric anaesthesia: a review. Paediatr Drugs. 1999;1:127–53.
Hatch DJ. New inhalation agents in paediatric anaesthesia. Br J Anaesth. 1999;83:42–9.
Keaney A, Diviney D, Harte S, Lyons B. Postoperative behavioral changes following anesthesia with sevoflurane. Pediatr Anesth. 2004;14:866–70.
Cohen IT, Finkel JC, Hannallah RS, Hummer KA, Patel KM. Rapid emergence does not explain agitation following sevoflurane anaesthesia in infants and children: a comparison with propofol. Paediatr Anaesth. 2003;13:63–7.
Sikich N, Lerman J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology. 2004;100:1138–45.
Kuratani N, Oi Y. Greater incidence of emergence agitation in children after sevoflurane anesthesia as compared with halothane: a meta-analysis of randomized controlled trials. Anesthesiology. 2008;109:225–32.
Weldon BC, Bell M, Craddock T. The effect of caudal analgesia on emergence agitation in children after sevoflurane versus halothane anesthesia. Anesth Analg. 2004;98:321–6.
Galinkin JL, Fazi LM, Cuy RM, Chiavacci RM, Kurth CD, Shah UK, Jacobs IN, Watcha MF. Use of intranasal fentanyl in children undergoing myringotomy and tube placement during halothane and sevoflurane anesthesia. Anesthesiology. 2000;93:1378–83.
Davis PJ, Greenberg JA, Gendelman M, Fertal K. Recovery characteristics of sevoflurane and halothane in preschool-aged children undergoing bilateral myringotomy and pressure equalization tube insertion. Anesth Analg. 1999;88:34–8.
Veyckemans F. Excitation phenomena during sevoflurane anaesthesia in children. Curr Opin Anesthesiol. 2001;14:339–43.
Aouad MT, Kanazi GE, Siddik-Sayyid SM, Gerges FJ, Rizk LB, Baraka AS. Preoperative caudal block prevents emergence agitation in children following sevoflurane anesthesia. Acta Anaesthesiol Scand. 2005;49:300–4.
Cohen IT, Hannallah RS, Hummer KA. The incidence of emergence agitation associated with desflurane anesthesia in children is reduced by fentanyl. Anesth Analg. 2001;93:88–91.
Komatsu H, Taie S, Endo S, Fukuda K, Ueki M, Nogaya J, Ogli K. Electrical seizures during sevoflurane anesthesia in two pediatric patients with epilepsy. Anesthesiology. 1994;81:1535–7.
Woodforth IJ, Hicks RG, Crawford MR, Stephen JP, Burke DJ. Electroencephalographic evidence of seizure activity under deep sevoflurane anesthesia in a nonepileptic patient. Anesthesiology. 1997;87:1579–82.
Constant I, Seeman R, Murat I. Sevoflurane and epileptiform EEG changes. Paediatr Anaesth. 2005;15:266–74.
Lapin SL, Auden SM, Goldsmith LJ, Reynolds AM. Effects of sevoflurane anaesthesia on recovery in children: a comparison with halothane. Paediatr Anaesth. 1999;9:299–304.
Ko YP, Huang CJ, Hung YC, Su NY, Tsai PS, Chen CC, Cheng CR. Premedication with low-dose oral midazolam reduces incidence and severity of emergence agitation in paediatric patients following sevoflurane anesthesia. Acta Anaesthesiol Sin. 2001;39:169–77.
McGraw T, Kendrick A. Oral midazolam premedication and postoperative behaviour in children. Paediatr Anaesth. 1998;8:117–21.
Breschan C, Platzer M, Jost R, Stettner H, Likar R. Midazolam does not reduce emergence delirium after sevoflurane anesthesia in children. Paediatr Anaesth. 2007;17:347–52.
Viitanen H, Annila P, Viitanen M, Tarkkila P. Premedication with midazolam delays recovery after ambulatory sevoflurane anesthesia in children. Anesth Analg. 1999;89:75–9.
Kulka PJ, Bressem M, Wiebalck A, Tryba M. Prevention of ‘postsevoflurane delirium’ with midazolam. Anaesthesist. 2001;50:401–5.
Schmidt AP, Valinetti EA, Bandeira D, Bertacchi MF, Simões CM, Auler JO Jr. Effects of preanesthetic administration of midazolam, clonidine, or dexmedetomidine on postoperative pain and anxiety in children. Paediatr Anaesth. 2007;17:667–74.
Yuen VM, Hui TW, Irwin MG, Yuen MK. A comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric anesthesia: a double-blinded randomized controlled trial. Anesth Analg. 2008;106:1715–21.
Isik B, Arslan M, Tunga AD, Kurtipek O. Dexmedetomidine decreases emergence agitation in pediatric patients after sevoflurane anesthesia without surgery. Paediatr Anaesth. 2006;16:748–53.
Claustrat B, Brun J, Chazot G. The basic physiology and pathophysiology of melatonin (physiological review). Sleep Med Rev. 2005;9:11–24.
Scheer FA, Czeisler CA. Melatonin, sleep, and circadian rhythms. Sleep Med Rev. 2005;9:5–9.
Jaffe SE, Patterson DR. Treating sleep problems in patients with burn injuries: practical considerations. J Burn Care Rehabil. 2004;25:294–305.
Petrie K, Cognaglen JV, Thompson L, Chamberlain K. Effect of melatonin on jet lag after long haul flights. BMJ. 1989;298:705–7.
Naguib M, Samarkandi AH. Premedication with melatonin: a double-blind, placebo controlled comparison with midazolam. Br J Anaesth. 1999;82:875–80.
Naguib M, Samarkandi AH. The comparative dose-response effect of melatonin and midazolam for premedication of adult patients: a double-blinded, placebo-controlled study. Anesth Analg. 2000;91:473–9.
Işık B, Baygin O, Bodur H. Premedication with melatonin vs. midazolam in anxious children. Paediatr Anaesth. 2008;18:635–41.
Samarkandi A, Naguib M, Riad W, Thalaj A, Alotibi W, Aldammas F, Albassam A. Melatonin vs. midazolam premedication in children: a double-blind, placebo-controlled study. Eur J Anaesthesiol. 2005;22:189–96.
Caumo W, Torres F, Moreira NL Jr, Auzani JA, Monteiro CA, Londero G, Ribeiro DF, Hidalgo MP. The clinical impact of preoperative melatonin on postoperative outcomes in patients undergoing abdominal hysterectomy. Anesth Analg. 2007;105:1263–71.
Kain ZN, MacLaren JE, Herrmann L, Mayes L, Rosenbaum A, Hata J, Lerman J. Preoperative melatonin and its effects on induction and emergence in children undergoing anesthesia and surgery. Anesthesiology. 2009;111:44–9.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Özcengiz, D., Gunes, Y. & Ozmete, O. Oral melatonin, dexmedetomidine, and midazolam for prevention of postoperative agitation in children. J Anesth 25, 184–188 (2011). https://doi.org/10.1007/s00540-011-1099-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-011-1099-2