
Abstract
Purpose
Critically ill cancer patients with sepsis represent a high-risk sub-group for the development of critical illness-related corticosteroid insufficiency (CIRCI); however, the incidence of CIRCI in this population is unknown. The purpose of this study was to determine the incidence of CIRCI in cancer patients with severe sepsis or septic shock.
Methods
A single-center, retrospective, observational study was conducted in a 52-bed medical–surgical intensive care unit of a National Cancer Institute-recognized academic oncology institution. Eighty-six consecutive patients with a diagnosis of severe sepsis or septic shock who received a high-dose 250-μg cosyntropin stimulation test were included. CIRCI was identified by a maximum delta serum cortisol of 9 μg/dL or less post cosyntropin.
Results
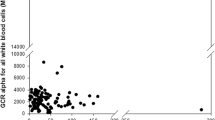
Overall, 59% (95% CI, 48–70%) of cancer patients with severe sepsis or septic shock were determined to have CIRCI. When compared to patients without CIRCI, patients with CIRCI had higher baseline serum cortisol (median, 26.3 versus 14.7 μg/dL; p = 0.002) and lower delta cortisol levels (median, 3.1 versus 12.5 μg/dL; p < 0.001). Mortality did not differ between the two groups. An inverse relationship was identified between baseline serum cortisol and maximum delta cortisol (maximum delta cortisol = −0.27 × baseline cortisol + 14.30; R 2 = 0.208, p < 0.001).
Conclusions
The incidence of CIRCI in cancer patients with severe sepsis or septic shock appears high. Further large-scale prospective trials are needed to confirm these findings.



Similar content being viewed by others


Abbreviations
- ACCM:
-
American College of Critical Care Medicine
- AI:
-
Adrenal insufficiency
- AMS:
-
Altered mental status
- APACHE:
-
Acute Physiology and Chronic Health Evaluation score
- BC:
-
Baseline serum cortisol
- CIRCI:
-
Critical illness-related corticosteroid insufficiency
- CORTICUS:
-
Corticosteroid Therapy of Septic Shock
- GI:
-
Gastrointestinal
- HPA:
-
Hypothalamus–pituitary–adrenal gland axis
- LOS:
-
Length of stay
- MDACC:
-
MD Anderson Cancer Center
- MDC:
-
Maximum delta cortisol
- MICU:
-
Medical intensive care unit
- OR:
-
Odds ratio
- SICU:
-
Surgical intensive care unit
References
Marik PE, Pastores SM, Annane D et al (2008) Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med 36:1937–1949
Rothwell PM, Udwadia ZF, Lawler PG (1991) Cortisol response to corticotropin and survival in septic shock. Lancet 337:582–583
Annane D, Sebille V, Troche G et al (2000) A 3-level prognostic classification in septic shock based on cortisol levels and cortisol response to corticotropin. JAMA 283:1038–1045
Annane D, Sebille V, Charpentier C et al (2002) Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 288:862–871
Oppert M, Schindler R, Husung C et al (2005) Low-dose hydrocortisone improves shock reversal and reduces cytokine levels in early hyperdynamic septic shock. Crit Care Med 33:2457–2464
Moran JL, Chapman MJ, O’Fathartaigh MS et al (1994) Hypocortisolaemia and adrenocortical responsiveness at onset of septic shock. Intensive Care Med 20:489–495
Bouachour G, Tirot P, Gouello JP et al (1995) Adrenocortical function during septic shock. Intensive Care Med 21:57–62
Briegel J, Schelling G, Haller M et al (1996) A comparison of the adrenocortical response during septic shock and after complete recovery. Intensive Care Med 22:894–899
Yildiz O, Doganay M, Aygen B et al (2002) Physiologic-dose steroid therapy in sepsis [ISRCTN36253388]. Crit Care 6:251–258
Bollaert PE, Fieux F, Charpentier C et al (2003) Baseline cortisol levels, cortisol response to corticotropin, and prognosis in late septic shock. Shock 19:13–15
Marik PE, Zaloga GP (2003) Adrenal insufficiency during septic shock. Crit Care Med 31:141–145
Manglik S, Flores E, Lubarsky L et al (2003) Glucocorticoid insufficiency in patients who present to the hospital with severe sepsis: a prospective clinical trial. Crit Care Med 31:1668–1675
Elsouri N, Bander J, Guzman JA (2006) Relative adrenal insufficiency in patients with septic shock; a close look to practice patterns. J Crit Care 21:73–78
Morel J, Venet C, Donati Y et al (2006) Adrenal axis function does not appear to be associated with hemodynamic improvement in septic shock patients systematically receiving glucocorticoid therapy. Intensive Care Med 32:1184–1190
Sprung CL, Annane D, Keh D et al (2008) Hydrocortisone therapy for patients with septic shock. N Engl J Med 358:111–124
Annane D, Bellissant E, Sebille V et al (1998) Impaired pressor sensitivity to noradrenaline in septic shock patients with and without impaired adrenal function reserve. Br J Clin Pharmacol 46:589–597
Sakai H, Yoshioka K, Yamagami K et al (2002) Complete adrenocorticotropin deficiency after radiation therapy for brain tumor with a normal growth hormone reserve. Intern Med 41:453–457
Schmiegelow M, Feldt-Rasmussen U, Rasmussen AK et al (2003) Assessment of the hypothalamo-pituitary-adrenal axis in patients treated with radiotherapy and chemotherapy for childhood brain tumor. J Clin Endocrinol Metab 88:3149–3154
Naing KK, Dewar JA, Leese GP (1999) Megestrol acetate therapy and secondary adrenal suppression. Cancer 86:1044–1049
Ron IG, Soyfer V, Goldray D et al (2002) A low-dose adrenocorticotropin test reveals impaired adrenal function in cancer patients receiving megestrol acetate therapy. Eur J Cancer 38:1490–1494
Rosenfield RL, Helke J, Lucky AW (1985) Dexamethasone preparation does not alter corticoid and androgen responses to adrenocorticotropin. J Clin Endocrinol Metab 60:585–589
Siraux V, De Backer D, Yalavatti G et al (2005) Relative adrenal insufficiency in patients with septic shock: comparison of low-dose and conventional corticotrophin tests. Crit Care Med 33:2479–2486
Cooper MS, Stewart PM (2003) Corticosteroid insufficiency in acutely ill patients. N Engl J Med 348:727–734
Hamrahian AH, Oseni TS, Arafah BM (2004) Measurements of serum free cortisol in critically ill patients. N Engl J Med 350:1629–1638
Annane D, Maxime V, Ibrahim F et al (2006) Diagnosis of adrenal insufficiency in severe sepsis and septic shock. Am J Respir Crit Care Med 174:1319–1326
Dellinger RP, Levy MM, Carlet JM et al (2008) Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock. Crit Care Med 36:296–327
Bruno JJ, Dee BM, Anderegg BA et al (2009) US practitioner opinions and prescribing practices regarding corticosteroid therapy for severe sepsis and septic shock (abstract). Crit Care Med 37(suppl):A241
Acknowledgments
The authors thank the medical and surgical ICU nursing staff for their invaluable support of this study.
Conflict of interest
The authors have no conflicts of interest regarding this publication.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bruno, J.J., Hernandez, M., Ghosh, S. et al. Critical illness-related corticosteroid insufficiency in cancer patients. Support Care Cancer 20, 1159–1167 (2012). https://doi.org/10.1007/s00520-011-1191-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-011-1191-z