
Abstract
Background
Primary hyperoxaluria (PH) is characterized by progressive chronic kidney disease (CKD) and systemic oxalate deposition. Myocardial dysfunction might be present early in the course of the disease. However, this hypothesis has not yet been tested in the PH population. Therefore, we aimed to determine whether strain imaging using two-dimensional speckle tracking echocardiography (2D-STE) might detect subclinical myocardial disease in otherwise asymptomatic PH patients.
Methods
Prospective study of pediatric and adolescent PH patients with preserved LV ejection fraction (LV EF) and without renal replacement therapy. Subjects underwent conventional echocardiography and 2D-STE. Global (GLS) and segmental peak systolic LV longitudinal strain (LS) measurements were obtained. Data were compared with age- and gender-matched controls, and Z-scores were calculated as appropriate.
Results
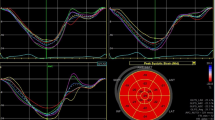
Fifteen PH patients (age 14.1 ± 5.9 years; 13/15 in CKD stages 1–2) were studied. Although LV EF was preserved (63 ± 6%) in patients, GLS was significantly impaired (GLS − 17.1 ± 2.2% vs − 22.4 ± 1.9%, p < 0.001). This was mainly due to decreased LS values in the apical segments (p < 0.05). Echocardiographic indices of ventricular wall thickness were significantly increased in patients compared to controls (all p < 0.03). GLS correlated significantly with Z-scores of diastolic interventricular wall thickness (r = − 0.57, p = 0.025) and moderately with serum creatinine levels (r = 0.53, p = 0.044). No correlation was found between GLS and blood pressure measurements.
Conclusions
Subclinical myocardial disease is already present early in the course of disease in PH patients with preserved LV EF and some degree of renal dysfunction, but without overt systemic oxalosis. Current recommendations to screen only PH patients with advanced CKD for cardiac disease should be revised accordingly.


Similar content being viewed by others


References
Hoppe B, Beck BB, Milliner DS (2009) The primary hyperoxalurias. Kidney Int 75:1264–1271. https://doi.org/10.1038/ki.2009.32
Cochat P, Rumsby G (2013) Primary hyperoxaluria. N Engl J Med 369:649–658. https://doi.org/10.1056/NEJMra1301564
Cochat P, Hulton SA, Acquaviva C, Danpure CJ, Daudon M, De Marchi M, Fargue S, Groothoff J, Harambat J, Hoppe B, Jamieson NV, Kemper MJ, Mandrile G, Marangella M, Picca S, Rumsby G, Salido E, Straub M, van Woerden CS (2012) Primary hyperoxaluria type 1: indications for screening and guidance for diagnosis and treatment. Nephrol Dial Transplant 27:1729–1736. https://doi.org/10.1093/ndt/gfs078
Beck BB, Hoyer-Kuhn H, Gobel H, Habbig S, Hoppe B (2013) Hyperoxaluria and systemic oxalosis: an update on current therapy and future directions. Expert Opin Investig Drugs 22:117–129. https://doi.org/10.1517/13543784.2013.741587
Mookadam F, Smith T, Jiamsripong P, Moustafa SE, Monico CG, Lieske JC, Milliner DS (2010) Cardiac abnormalities in primary hyperoxaluria. Circ J 74:2403–2409
Lagies R, Beck BB, Hoppe B, Sreeram N, Udink ten Cate FE (2013) Apical sparing of longitudinal strain, left ventricular rotational abnormalities, and short-axis dysfunction in primary hyperoxaluria type 1. Circ Heart Fail 6:e45–e47. https://doi.org/10.1161/circheartfailure.113.000432
Palka P, Duhig E, Carey L, Galbraith A (2001) Primary oxalosis with cardiac involvement: echocardiographic features of an unusual form of cardiomyopathy. Circulation 103:E122–E123
Yoshioka J, Park YD, Tanaka Y, Kobayashi Y, Miyajima M, Tani A, Hori M, Shirai D (2001) Echocardiographic features in a patient with primary oxalosis. Echocardiography 18:599–602
Schulze MR, Wachter R, Schmeisser A, Fischer R, Strasser RH (2006) Restrictive cardiomyopathy in a patient with primary hyperoxaluria type II. Clin Res Cardiol 95:235–240. https://doi.org/10.1007/s00392-006-0362-2
Kalam K, Otahal P, Marwick TH (2014) Prognostic implications of global LV dysfunction: a systematic review and meta-analysis of global longitudinal strain and ejection fraction. Heart 100:1673–1680. https://doi.org/10.1136/heartjnl-2014-305538
Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K, Yusuf S, Granger CB, Michelson EL, Wang D, Pocock S, Pfeffer MA (2005) Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 112:3738–3744. https://doi.org/10.1161/circulationaha.105.561423
Collier P, Phelan D, Klein A (2017) A test in context: myocardial strain measured by speckle-tracking echocardiography. J Am Coll Cardiol 69:1043–1056. https://doi.org/10.1016/j.jacc.2016.12.012
Krishnasamy R, Isbel NM, Hawley CM, Pascoe EM, Leano R, Haluska BA, Stanton T (2014) The association between left ventricular global longitudinal strain, renal impairment and all-cause mortality. Nephrol Dial Transplant 29:1218–1225. https://doi.org/10.1093/ndt/gfu004
Lagies R, Beck BB, Hoppe B, Sheta SS, Weiss V, Sreeram N, Udink ten Cate FE (2015) Inhomogeneous longitudinal cardiac rotation and impaired left ventricular longitudinal strain in children and young adults with end-stage renal failure undergoing hemodialysis. Echocardiography 32:1250–1260. https://doi.org/10.1111/echo.12842
Neuhauser HK, Thamm M, Ellert U, Hense HW, Rosario AS (2011) Blood pressure percentiles by age and height from nonoverweight children and adolescents in Germany. Pediatrics 127:e978–e988. https://doi.org/10.1542/peds.2010-1290
Schwartz GJ, Brion LP, Spitzer A (1987) The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediat Clin North Am 34:571–590
Hoppe B, Kemper MJ, Bokenkamp A, Langman CB (1998) Plasma calcium-oxalate saturation in children with renal insufficiency and in children with primary hyperoxaluria. Kidney Int 54:921–925. https://doi.org/10.1046/j.1523-1755.1998.00066.x
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 28:1–39.e14. https://doi.org/10.1016/j.echo.2014.10.003
Kampmann C, Wiethoff CM, Wenzel A, Stolz G, Betancor M, Wippermann CF, Huth RG, Habermehl P, Knuf M, Emschermann T, Stopfkuchen H (2000) Normal values of M mode echocardiographic measurements of more than 2000 healthy infants and children in central. Eur Heart 83:667–672
Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N (1986) Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 57:450–458
Daniels SR, Meyer RA, Liang YC, Bove KE (1988) Echocardiographically determined left ventricular mass index in normal children, adolescents and young adults. J Am Coll Cardiol 12:703–708
de Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, de Divitiis O, Alderman MH (1992) Left ventricular mass and body size in normotensive children and adults: assessment of allometric relations and impact of overweight. J Am Coll Cardiol 20:1251–1260
Matteucci MC, Wuhl E, Picca S, Mastrostefano A, Rinelli G, Romano C, Rizzoni G, Mehls O, de Simone G, Schaefer F (2006) Left ventricular geometry in children with mild to moderate chronic renal insufficiency. J Am Soc Nephrol 17:218–226. https://doi.org/10.1681/asn.2005030276
Marcus KA, Mavinkurve-Groothuis AMC, Barends M, van Dijk A, Feuth T, de Korte C, Kapusta L (2011) Reference values for myocardial two-dimensional strain echocardiography in a healthy pediatric and young adult cohort. J Am Soc Echocardiogr 24:625–636
Potter E, Marwick TH (2018) Assessment of left ventricular function by echocardiography: the case for routinely adding global longitudinal strain to ejection fraction. JACC Cardiovasc Imaging 11:260–274. https://doi.org/10.1016/j.jcmg.2017.11.017
Panoulas VF, Sulemane S, Konstantinou K, Bratsas A, Elliott SJ, Dawson D, Frankel AH, Nihoyannopoulos P (2015) Early detection of subclinical left ventricular myocardial dysfunction in patients with chronic kidney disease. Eur Heart J Cardiovasc Imaging 16:539–548. https://doi.org/10.1093/ehjci/jeu229
Krishnasamy R, Isbel NM, Hawley CM, Pascoe EM, Burrage M, Leano R, Haluska BA, Marwick TH, Stanton T (2015) Left ventricular global longitudinal strain (GLS) is a superior predictor of all-cause and cardiovascular mortality when compared to ejection fraction in advanced chronic kidney disease. PLoS One 10:e0127044. https://doi.org/10.1371/journal.pone.0127044
Edwards NC, Moody WE, Yuan M, Hayer MK, Ferro CJ, Townend JN, Steeds RP (2015) Diffuse interstitial fibrosis and myocardial dysfunction in early chronic kidney disease. Am J Cardiol 115:1311–1317. https://doi.org/10.1016/j.amjcard.2015.02.015
Hayer MK, Price AM, Liu B, Baig S, Ferro CJ, Townend JN, Steeds RP, Edwards NC (2018) Diffuse myocardial interstitial fibrosis and dysfunction in early chronic kidney disease. Am J Cardiol 121:656–660. https://doi.org/10.1016/j.amjcard.2017.11.041
Winterberg PD, Jiang R, Maxwell JT, Wang B, Wagner MB (2016) Myocardial dysfunction occurs prior to changes in ventricular geometry in mice with chronic kidney disease (CKD). Phys Rep 4:e12732. https://doi.org/10.14814/phy2.12732
Mulay SR, Eberhard JN, Pfann V, Marschner JA, Darisipudi MN, Daniel C, Romoli S, Desai J, Grigorescu M, Kumar SV, Rathkolb B, Wolf E, Hrabe de Angelis M, Bauerle T, Dietel B, Wagner CA, Amann K, Eckardt KU, Aronson PS, Anders HJ, Knauf F (2016) Oxalate-induced chronic kidney disease with its uremic and cardiovascular complications in C57BL/6 mice. Am J Physiol Ren Physiol 310:F785–f795. https://doi.org/10.1152/ajprenal.00488.2015
Massie BM, Bharati S, Scheinman MM, Lev M, Desai J, Rubeson E, Schmidt W (1981) Primary oxalosis with pan-conduction cardiac disease: electrophysiologic and anatomic correlation. Circulation 64:845–852
Coltart DJ, Hudson RE (1971) Primary oxalosis of the heart: a cause of heart block. Br Heart J 33:315–319
Liu YW, Su CT, Huang YY, Yang CS, Huang JW, Yang MT, Chen JH, Tsai WC (2011) Left ventricular systolic strain in chronic kidney disease and hemodialysis patients. Am J Nephrol 33:84–90
Demetgul H, Giray D, Delibas A, Hallioglu O (2018) 2D-speckle tracking echocardiography contributes to early identification of impaired left ventricular myocardial function in children with chronic kidney disease. Cardiol Young 28:1404–1409
Weaver DJ Jr, Mitsnefes MM (2018) Cardiovascular disease in children and adolescents with chronic kidney disease. Semin Nephrol 38:559–569
Weaver DJ Jr, Kimball T, Witt SA, Glascock BJ, Khoury PR, Kartal J, Mitsnefes MM (2008) Subclinical systolic dysfunction in pediatric patients with chronic kidney disease. J Pediatr 153:565–569
Senapati A, Sperry BW, Grodin JL, Kusunose K, Thavendiranathan P, Jaber W, Collier P, Hanna M, Popovic ZB, Phelan D (2016) Prognostic implication of relative regional strain ratio in cardiac amyloidosis. Heart 102:748–754. https://doi.org/10.1136/heartjnl-2015-308657
Phelan D, Collier P, Thavendiranathan P, Popovic ZB, Hanna M, Plana JC, Marwick TH, Thomas JD (2012) Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis. Heart 98:1442–1448. https://doi.org/10.1136/heartjnl-2012-302353
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lagies, R., Udink ten Cate, F.E.A., Feldkötter, M. et al. Subclinical myocardial disease in patients with primary hyperoxaluria and preserved left ventricular ejection fraction: a two-dimensional speckle-tracking imaging study. Pediatr Nephrol 34, 2591–2600 (2019). https://doi.org/10.1007/s00467-019-04330-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-019-04330-7