
Abstract
Background
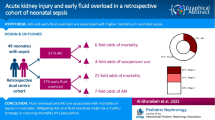
Acute kidney injury (AKI) is common and portends mortality in several neonatal cohorts. Fluid overload is independently associated with poor outcomes in children and adults but has not been extensively studied in neonates.
Methods
Between February 2010 and May 2011, we followed 58 neonates who met the following criteria: birth weight >2,000 g, gestational age ≥34 weeks, 5-min Apgar ≤7, and parental consent. Serum creatinine (SCr) was measured daily for first 4 days of life. AKI was defined as a rise in SCr of > 0.3 mg/dl or persistent SCr above 1.5 mg/dl.
Results
AKI was present in 9/58 (15.6 %) neonates and was associated with higher birth weight, being male, lower 5-min Apgar scores, lower cord pH, delivery room intubation, and absence of maternal pre-eclampsia. Percent weight accumulation at day 3 of life was higher in those with AKI [median = 8.2, interquartile range (IQR) = 4.4–21.6)] than without AKI (median = −4 (IQR = −6.5 to 0.0) (p < 0.001). Infants with AKI had lower survival rates than those without AKI [7/9 (72 %) vs. 49/49 (100 %) (p < 0.02)].
Conclusions
AKI incidence in this neonatal population is similar to other neonatal cohorts. Near-term/term infants with AKI have a higher mortality rate and a net positive fluid balance over the first few days of life.



Similar content being viewed by others


References
Koralkar R, Ambalavanan N, Levitan EB, McGwin G, Goldstein S, Askenazi D (2011) Acute kidney injury reduces survival in very low birth weight infants. Pediatr Res 69:354–358
Selewski DT, Jordan B, Dechert RE, Sarkar S (2012) Acute Kidney Injury in Asphyxiated Newborns Treated with Therapeutic Hypothermia. J Pediatr. doi:10.1016/j.jpeds.2012.10.002
Gadepalli SK, Selewski DT, Drongowski RA, Mychaliska GB (2011) Acute kidney injury in congenital diaphragmatic hernia requiring extracorporeal life support: an insidious problem. J Pediar Sur g 46:630–635
Blinder JJ, Goldstein SL, Lee VV, Baycroft A, Fraser CD, Nelson D, Jefferies JL (2012) Congenital heart surgery in infants: effects of acute kidney injury on outcomes. J Thorac Cardiovasc Surg 143:368–374
Askenazi DJ, Ambalavanan N, Hamilton K, Cutter G, Laney D, Kaslow R, Georgeson K, Barnhart DC, Dimmitt RA (2011) Acute kidney injury and renal replacement therapy independently predict mortality in neonatal and pediatric noncardiac patients on extracorporeal membrane oxygenation. Pediatr Crit Care Med 12:e1–e6
Askenazi DJ, Feig DI, Graham NM, Hui-Stickle S, Goldstein SL (2006) 3–5 year longitudinal follow-up of pediatric patients after acute renal failure. Kidney Int 69:184–189
Mammen C, Al Abbas A, Skippen P, Nadel H, Levine D, Collet JP, Matsell DG (2012) Long-term risk of CKD in children surviving episodes of acute kidney injury in the intensive care unit: a prospective cohort study. Am J Kidney Dis 59:523–530
Coca SG, Singanamala S, Parikh CR (2012) Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int 81:442–448
Mathews TJ, MacDorman MF (2011) Infant mortality statistics from the 2007 period linked birth/infant death data set. National vital statistics reports : from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System 59:1–30
Arikan AA, Zappitelli M, Goldstein SL, Naipaul A, Jefferson LS, Loftis LL (2012) Fluid overload is associated with impaired oxygenation and morbidity in critically ill children. Pediatr Crit Care Med 13:253–258
Hayes LW, Oster RA, Tofil NM, Tolwani AJ (2009) Outcomes of critically ill children requiring continuous renal replacement therapy. J Crit Care 24:394–400
Sutherland SM, Zappitelli M, Alexander SR, Chua AN, Brophy PD, Bunchman TE, Hackbarth R, Somers MJ, Baum M, Symons JM, Flores FX, Benfield M, Askenazi D, Chand D, Fortenberry JD, Mahan JD, McBryde K, Blowey D, Goldstein SL (2010) Fluid overload and mortality in children receiving continuous renal replacement therapy: the prospective pediatric continuous renal replacement therapy registry. Am J Kidney Dis 55:316–325
Fulop T, Pathak MB, Schmidt DW, Lengvarszky Z, Juncos JP, Lebrun CJ, Brar H, Juncos LA (2010) Volume-related weight gain and subsequent mortality in acute renal failure patients treated with continuous renal replacement therapy. ASAIO J 56:333–337
Sakr Y, Vincent JL, Reinhart K, Groeneveld J, Michalopoulos A, Sprung CL, Artigas A, Ranieri VM (2005) High tidal volume and positive fluid balance are associated with worse outcome in acute lung injury. Chest 128:3098–3108
Upadya A, Tilluckdharry L, Muralidharan V, Amoateng-Adjepong Y, Manthous CA (2005) Fluid balance and weaning outcomes. J Intensive Care Med 31:1643–1647
Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL (2006) Comparison of two fluid-management strategies in acute lung injury. New Engl J Med 354:2564–2575
Bagshaw SM, Wald R, Barton J, Burns KE, Friedrich JO, House AA, James MT, Levin A, Moist L, Pannu N, Stollery DE, Walsh MW (2012) Clinical factors associated with initiation of renal replacement therapy in critically ill patients with acute kidney injury-a prospective multicenter observational study. J Crit Care 27:268–275
Heung M, Wolfgram DF, Kommareddi M, Hu Y, Song PX, Ojo AO (2012) Fluid overload at initiation of renal replacement therapy is associated with lack of renal recovery in patients with acute kidney injury. Nephrol Dial Transplant 27:956–961
Schmidt B, Roberts RS, Fanaroff A, Davis P, Kirpalani HM, Nwaesei C, Vincer M, Investigators T (2006) Indomethacin prophylaxis, patent ductus arteriosus, and the risk of bronchopulmonary dysplasia: further analyses from the Trial of Indomethacin Prophylaxis in Preterms (TIPP). J Pediatr 148:730–734
Marshall DD, Kotelchuck M, Young TE, Bose CL, Kruyer L, O’Shea TM (1999) Risk factors for chronic lung disease in the surfactant era: a North Carolina population-based study of very low birth weight infants. North Carolina Neonatologists Association. Pediatrics 104:1345–1350
Endre ZH (2011) Renal ischemic preconditioning: finally some good news for prevention of acute kidney injury. Kidney Int 80:796–798
Zimmerman RF, Ezeanuna PU, Kane JC, Cleland CD, Kempananjappa TJ, Lucas FL, Kramer RS (2011) Ischemic preconditioning at a remote site prevents acute kidney injury in patients following cardiac surgery. Kidney Int 80:861–867
Venugopal V, Laing CM, Ludman A, Yellon DM, Hausenloy D (2010) Effect of remote ischemic preconditioning on acute kidney injury in nondiabetic patients undergoing coronary artery bypass graft surgery: a secondary analysis of 2 small randomized trials. Am J Kidney DIs 56:1043–1049
Jetton JG, Askenazi DJ (2012) Update on acute kidney injury in the neonate. Curr Opin Pediatr 24:191–196
Selewski DT, Cornell TT, Lombel RM, Blatt NB, Han YY, Mottes T, Kommareddi M, Kershaw DB, Shanley TP, Heung M (2011) Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med 37:1166–1173
Funding source
This study was supported by grants provided by the American Society of Nephrology Career Development Grant, the Kaul Pediatric Research Institute and a pilot and feasibility grant from the NIH-sponsored O’Brien Center for Acute Kidney Injury Research (www.obrienaki.org). Dr. Askenazi is a consultant and serves as a speaker for Gambro Renal Products.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Askenazi, D.J., Koralkar, R., Hundley, H.E. et al. Fluid overload and mortality are associated with acute kidney injury in sick near-term/term neonate. Pediatr Nephrol 28, 661–666 (2013). https://doi.org/10.1007/s00467-012-2369-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-012-2369-4