
Abstract
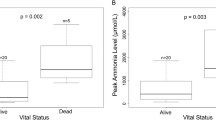
In a 10-year review of the utilization of continuous veno-venous hemofiltration (CVVH) for the treatment of neonatal hyperammonemia, 14 patients were identified with hyperammonemia due to either a urea cycle defect or an organic acidemia. Intensive care survival was 64%. The pretreatment level of serum ammonia and the rapidity of ammonia clearance did not differ between survivors and non-survivors (p = 0.16 and p = 0.93, respectively). Likewise, the duration of CVVH therapy did not differ between survivors and non-survivors (p = 0.1). Indicators of pretreatment physiological stress showed either a correlation with non-survival [Pediatric Risk of Mortality (PRISM) score, p = 0.006, cardioactive drug requirement, p = 0.003], or demonstrated a trend to such a correlation (serum lactate, p = 0.06). Complications associated with the CVVH technique were infrequent. Hypotension was seen in seven patients, but in only one patient did it arise de novo following the initiation of CVVH. In conclusion, neither the severity of the hyperammonemic state nor the efficacy of ammonia removal correlated with patient outcome. The pre-CVVH PRISM score and requirement for cardio-active medication were significantly greater in those patients who did not survive their acute illness. The pre-CVVH physiological condition of the neonates in this cohort was the main determinant of outcome.
Similar content being viewed by others


References
Butterworth RF (1998) Effects of hyperammonaemia on brain function. J Inherit Metab Dis 21(Suppl 1):6–20
Cagnon L, Braissant O (2007) Hyperammonaemia induced toxicity for the developing central nervous system. Brain Res Rev 56:183–197
Schaefer F, Straube E, Oh J, Mehls O, Mayatepak E (1999) Dialysis in neonates with inborn errors of metabolism. Nephrol Dial Transplant 14:910–918
Picca S, Dionisi-Vici C, Abeni D, Pastore A, Rizzo C, Orzalesi M, Sabetta G, Rizzoni G, Bartuli A (2001) Extracorporeal dialysis in neonatal hyperammonemia: modalities and prognostic indicators. Pediatr Nephrol 16:862–867
Batshaw ML, Brusilow S, Waber L, Blom W, Brubakk AM, Burton BK, Cann HM, Kerr D, Mamunes P, Matalon R, Myerberg D, Schafer IA (1982) Treatment of inborn errors of urea synthesis: activation of alternative pathways of waste nitrogen synthesis and excretion. N Engl J Med 306:1387–1392
Rajpoot DK, Gargus JJ (2004) Acute hemodialysis for hyperammonemia in small neonates. Pediatr Nephrol 19:390–395
McBryde KD, Kershaw DB, Bunchman TE, Maxvold NJ, Mottes TA, Kudelka TL, Brophy PD (2006) Renal replacement therapy in the treatment of confirmed or suspected inborn errors of metabolism. J Pediatr 148:770–778
Enns GM, Berry SA, Berry GT, Rhead WJ, Brusilow SW, Hamosh A (2007) Survival after treatment with phenylacetate and benzoate for urea-cycle disorders. N Engl J Med 356:2282–2292
Bunchman TE, Barletta G-M, Winters JW, Gardner JJ, Crumb TL, McBryde KD (2007) Phenylacetate and benzoate clearance in a hyperammonemic infant on sequential hemodialysis and hemofiltration. Pediatr Nephrol 22:1062–1065
Sadowski RH, Harmon WE, Jabs K (1994) Acute hemodialysis of infants weighing less than five kilograms. Kidney Int 45:903–906
Arbeiter AK, Kranz B, Wingen A-M, Bonzel K-E, Dohna-Schwake C, Hanssler L, Neudorf U, Hoyer PF, Buscher R (2010) Continuous venovenous haemodialysis (CVVHD) and continuous peritoneal dialysis (CPD) in the acute management of 21 children with inborn errors of metabolism. Nephrol Dial Transplant 25:1257–1265
Avanoglu A, Ergun O, Bakirtas F, Erdener A (1997) Characteristics of multisystem organ failure in neonates. Eur J Pediatr Surg 7:263–266
Goldstein SL, Currier H, Graf JM, Cosio CC, Brewer ED, Sachdeva R (2001) Outcome of children receiving continuous venovenous haemofiltration. Pediatrics 107:1309–1312
Ponikvar R, Kandus A, Urbancic A, Kornhauser AG, Primozic J, Ponikvar JB (2002) Continuous renal replacement therapy and plasma exchange in newborns and infants. Artif Organs 26:163–168
Hothi DK, St George-Hyslop C, Geary D, Bohn D, Harvey E (2006) Continuous renal replacement therapy (CRRT) in children using the AQUARIUSTM. Nephrol Dial Transplant 21:2296–2300
Fernández C, López-Herce J, Flores JC, Galaviz D, Rupérez M, Brandstrup KB, Bustinza A (2005) Prognosis in critically ill children requiring continuous renal replacement therapy. Pediatr Nephrol 20:1473–1477
Bunchman TE, McBryde KD, Mottes TE, Gardner JJ, Maxvold NJ, Brophy PD (2001) Pediatric acute renal failure: outcome by modality and disease. Pediatr Nephrol 16:1067–1071
Brophy PD, Mottes TA, Kudelka TL, McBryde KD, Gardner JJ, Maxvold NJ, Bunchman TE (2001) AN-69 membrane reactions are pH-dependent and preventable. Am J Kidney Dis 38:173–178
Chan WKY, But WM, Law CW (2002) Ammonia detoxification by continuous venovenous haemofiltration in an infant with urea cycle defect. Hong Kong Med J 8:207–210
Lai YC, Huang HP, Tsai IJ, Tsau YK (2007) High-volume continuous venovenous hemofiltration as an effective therapy for acute management of inborn errors of metabolism in young children. Blood Purif 25:303–308
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Westrope, C., Morris, K., Burford, D. et al. Continuous hemofiltration in the control of neonatal hyperammonemia: a 10-year experience. Pediatr Nephrol 25, 1725–1730 (2010). https://doi.org/10.1007/s00467-010-1549-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-010-1549-3