
Abstract
Background
The ability to adequately train surgical residents in flexible and rigid endoscopy has become a difficult challenge for program directors. The American Board of Surgery requires residents to be familiar in these procedures but the methods for training have not been well defined nor formally outlined. The goals of this study were to evaluate resident experience in flexible endoscopy and laparoscopy and to investigate the specific methods used by surgical programs for the training of residents.
Methods
A survey was created by the authors and the Resident Education Committee of the Society of American Gastrointestinal Endoscopic Surgeons and was mailed to all program directors in general surgery in the United States based on the data base of the Association of Program Directors in Surgery (APDS).
Results
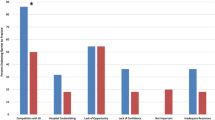
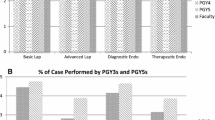
Ninety-six of 283 surveys were returned (33.9%). The surgeon played a greater role in flexible endoscopic training in 1998 as compared to 1988 (p=0.002). When analyzed by type of institution, community programs showed a similar trend but this was not seen in academic programs. Formal endoscopy rotations existed in 60% of programs but flexible endoscopy (5.2%) and laparoscopy (10.4%) fellowships were uncommon. No significant differences in the number of advanced laparoscopic procedures performed were found between academic and community programs. The presence of a laparoscopic fellow did not significantly decrease the number of cases per resident.
Conclusion
According to our survey, surgery departments have a greater impact on flexible endoscopic training in 1998 than in 1988. This is likely due to the creation of formal endoscopy rotations and the hiring of fellowship trained endoscopic instructors. In addition, community programs have been able to provide adequate experience in both basic and advanced laparoscopic techniques as compared to academic programs. As with flexible endoscopy, however, formal laparoscopic rotations may be necessary to allow more intensive experience for each resident.
Similar content being viewed by others

References
American Board of Surgery (1986–1987) The Booklet of Information., Philadelphia, pp
Cosgrove JM, Margolis IB, Riou JP, Wait RB (1993) Formal endoscopy training for senior and junior house staff. J Laparoendosc Surg 3: 525–529
Cullado MJ, Porter JA, Slezak FA (1991) The evolution of surgical endoscopic training: Meeting the American Board of Surgery Requirements. Am Surg 57: 250–253
Hawasli A, Featherstone R, Lloyd L, Vorhees M (1996) Laparoscopic training in residency program. J Lapraroendosc Surg 6: 171–174
Larson GM, Mullins RJ, Wieman TJ, Polk Jr HC (1988) Evaluation of endoscopy training in a general surgery residency. Am Surg 54: 64–67
Marshall JB (1995) Technical proficiency of trainees performing colonoscopy: a learning curve. Gastrointest Endosc 42: 287–291
Max MH, Polk Jr HC (1982) Perceived needs for gastrointestinal endoscopic training in surgical residencies. Am J Surg 143: 150–154
Mellinger JD, Ponsky JL (1994) Surgical endoscopy fellowships: what difference do they make? Surg Endosc 8: 86–89
Myers JO, Ragland JJ, Candelaria LA (1990) Fiberoptic endoscopy of the gastrointestinal tract in surgical training. Surg Gynecol Obstet 170: 283–286
Reed DN, Collins JD, Wyatt WJ, Hull JE, Patton ML, Dahm SO, Dabideen HH, Hudson JC, Allen DB (1992) Can general surgeons perform colonoscopy safely? Am J Surg 163: 257–259
Rodning CB, Zingarelli WJ, Webb WR, Curreri PW (1986) Postgraduate surgical flexible endoscopic education. Ann Surg 203: 272–274
SAGES Integrating advanced laparoscopy into surgical residency training. Surg Endosc 12: 374–376
Schauer PR, Schwesinger WH, Page CP, Stewart R, Levine BA, Sirinek KR (1997) Complications of surgical endoscopy: a decade of experience from a surgical residency training program. Surg Endosc 11: 8–11
Scott-Conner CEH, Hall TJ, Anglin BL, Muakkassa FF, Poole GV, Thompson AR, Wilton PB (1994) The integration of laparoscopy into a surgical residency and implications for the training environment. Surg Endosc 8: 1054–1057
Smale BF, Reber HA, Terry BE, Silver D (1983) The creation of a surgical endoscopy training program: Is there sufficient clinical material? Surgery 94: 180–185
Unger SW, Satava RM, Scott JS (1992) Resident education in surgical endoscopy. Am Surg 58: 643–646
Author information
Authors and Affiliations
Additional information
Online publication: 12 June 2001
Rights and permissions
About this article
Cite this article
Marks, J.M., Nussbaum, M.S., Pritts, T.A. et al. Evaluation of endoscopic and laparoscopic training practices in surgical residency programs. Surg Endosc 15, 1011–1015 (2001). https://doi.org/10.1007/s004640080082
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s004640080082