
Abstract
Introduction
Technical variation exists when performing the gastrojejunostomy during Roux-en-Y gastric bypass (RYGB). However, it is unclear whether changing technique results in improved outcomes or patient harm.
Methods
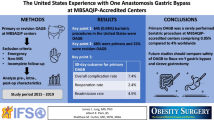
Surgeons participating in a state-wide bariatric surgery quality collaborative who completed a survey on how they perform a typical RYGB in 2011 and again in 2021 were included in the analysis (n = 31). Risk-adjusted 30-day complication rates and case characteristics for cases in 2011 were compared to those in 2021 among surgeons who changed their gastrojejunostomy technique from end-to-end anastomosis (EEA) to either a linear staple or handsewn anastomosis (LSA/HSA). In addition, case characteristics and outcomes among surgeons who maintained an EEA technique throughout the study period were assessed.
Results
A total of 15 surgeons (48.3%) changed their technique from EEA to LSA/HSA while 7 surgeons (22.3%) did not. Nine surgeons did LSA or HSA the entire period and therefore were not included. Surgeons who changed their technique had significantly lower rates of surgical complications in 2021 when compared to 2011 (1.9% vs 5.1%, p = 0.0015), including lower rates of wound complications (0.5% vs 2.1%, p = 0.0030) and stricture (0.1% vs 0.5%, p = 0.0533). Likewise, surgeons who did not change their EEA technique, also experienced a decrease in surgical complications (1.8% vs 5.8%, p < 0.0001), wound complications (0.7% vs 2.1%, p < 0.0001) and strictures (0.2% vs 1.2%, p = 0.0006). Surgeons who changed their technique had a significantly higher mean annual robotic bariatric volume in 2021 (30.0 cases vs 4.9 cases, p < 0.0001) when compared to those who did not.
Conclusions
Surgeons who changed their gastrojejunostomy technique from circular stapled to handsewn demonstrated greater utilization of the robotic platform than those who did not and experienced a similar decrease in adverse events during the study period, despite altering their technique. Surgeons who chose to modify their operative technique may be more likely to adopt newer technologies.
Graphical abstract




Similar content being viewed by others


Abbreviations
- EEA:
-
End-to-end anastomosis
- GJ:
-
Gastrojejunostomy
- HAS:
-
Hand sewing anastomosis
- LSA:
-
Linear stapler anastomosis
- MBSC:
-
Michigan Bariatric Surgical Collaborative
- RYGB:
-
Roux-en-Y gastric bypass
References
Major P, Stefura T, Walędziak M, Janik M, Pędziwiatr M, Wysocki M, Rubinkiewicz M, Witowski J, Szeliga J, Budzyński A (2019) What makes bariatric operations difficult-results of a national survey. Medicina 55(6):218. https://doi.org/10.3390/medicina55060218
Fehervari M, Alyaqout K, Lairy A, Khwaja H, Bonanomi G, Efthimiou E (2021) Gastrojejunal anastomotic technique does it matter: weight loss and weight regain 5 years after laparoscopic Roux-en-Y gastric bypass. Obes Surg 31(1):267–273. https://doi.org/10.1007/s11695-020-04932-3
Fringeli Y, Worreth M, Langer I (2015) Gastrojejunal anastomosis complications and their management after laparoscopic Roux-en-Y gastric bypass. J Obes 2015:698425. https://doi.org/10.1155/2015/698425
Espinel J, Pinedo E (2012) Stenosis in gastric bypass: endoscopic management. World J Gastrointest Endosc 4(7):290–295. https://doi.org/10.4253/wjge.v4.i7.290
Shope TR, Cooney RN, McLeod J, Miller CA, Haluck RS (2003) Early results after laparoscopic gastric bypass: EEA vs GIA stapled gastrojejunal anastomosis. Obes Surg 13(3):355–359. https://doi.org/10.1381/096089203765887651
Hider AM, Bonham AJ, Carlin AM, Finks JF, Ghaferi AA, Varban OA, Ehlers AP (2022) Impact of concurrent hiatal hernia repair during laparoscopic sleeve gastrectomy on patient-reported gastroesophageal reflux symptoms: a state-wide analysis. Surg Obes Relat Dis. https://doi.org/10.1016/j.soard.2022.12.021
Fakas S, Elias M, Lim D, Meytes V (2021) Comparison of gastrojejunostomy techniques and anastomotic complications: a systematic literature review. Surg Endosc 35(12):6489–6496. https://doi.org/10.1007/s00464-020-08142-x
Jiang HP, Lin LL, Jiang X, Qiao HQ (2016) Meta-analysis of hand-sewn versus mechanical gastrojejunal anastomosis during laparoscopic Roux-en-Y gastric bypass for morbid obesity. Int J Surg 32:150–157. https://doi.org/10.1016/j.ijsu.2016.04.024
Abellán I, López V, Lujan J, Abrisqueta J, Hernández Q, Frutos MD, Parrilla P (2015) Stapling versus hand suture for gastroenteric anastomosis in Roux-en-Y gastric bypass: a randomized clinical trial. Obes Surg 25(10):1796–1801. https://doi.org/10.1007/s11695-015-1638-2
Khalayleh H, Pines G, Imam A, Sapojnikov S, Buyeviz V, Mavor E (2018) Anastomotic stricture rates following Roux-en-Y gastric bypass for morbid obesity: a comparison between linear and circular-stapled anastomosis. J Laparoendosc Adv Surg Tech A 28(6):631–636. https://doi.org/10.1089/lap.2017.0619
Penna M, Markar SR, Venkat-Raman V, Karthikesalingam A, Hashemi M (2012) Linear-stapled versus circular-stapled laparoscopic gastrojejunal anastomosis in morbid obesity: meta-analysis. Surg Laparosc Endosc Percutan Tech 22(2):95–101. https://doi.org/10.1097/SLE.0b013e3182470f38
Baccaro LM, Vunnamadala K, Sakharpe A, Wilhelm BJ, Aksade A (2015) Stricture rate after laparoscopic Roux-en-Y gastric bypass with a 21-mm circular stapler versus a 25-mm linear stapler. Bariatr Surg Pract Patient Care 10(1):33–37. https://doi.org/10.1089/bari.2014.0048
Suggs WJ, Kouli W, Lupovici M, Chau WY, Brolin RE (2007) Complications at gastrojejunostomy after laparoscopic Roux-en-Y gastric bypass: comparison between 21- and 25-mm circular staplers. Surg Obes Relat Dis 3(5):508–514. https://doi.org/10.1016/j.soard.2007.05.003
Fisher BL, Atkinson JD, Cottam D (2007) Incidence of gastroenterostomy stenosis in laparoscopic Roux-en-Y gastric bypass using 21- or 25-mm circular stapler: a randomized prospective blinded study. Surg Obes Relat Dis 3(2):176–179. https://doi.org/10.1016/j.soard.2006.11.014
Garcia Cabrera AT, Romero-Velez G, Pereira X, Vazzana JT, Camacho DR (2022) Decreasing surgical site infection associated with the use of circular staplers during Roux-En-Y gastric bypass. J Soc Laparosc Robot Surg 26(4):e202200056. https://doi.org/10.4293/JSLS.2022.00056
Birkmeyer JD, Finks JF, Oreilly A, Oerline M, Carlin AM, Nunn AR, Dimick J, Banerjee M, Birkmeyer NJ, Michigan Bariatric Surgery Collaborative (2013) Surgical skill and complication rates after bariatric surgery. N Engl J Med 369(15):1434–1442. https://doi.org/10.1056/NEJMsa1300625
Julià D, Gómez N, Codina-Cazador A (2014) Surgical skill and complication rates after bariatric surgery. N Engl J Med 370(3):285. https://doi.org/10.1056/NEJMc1313890
Dimick JB, Varban OA (2015) Surgical video analysis: an emerging tool for improving surgeon performance. BMJ Qual Saf 24(8):490–491. https://doi.org/10.1136/bmjqs-2015-004439
Varban OA, Cain-Nielsen AH, Wood MH, Carlin AM, Ghaferi AA, Telem DA (2022) Adopt or abandon? Surgeon-specific trends in robotic bariatric surgery utilization between 2010 and 2019. J Laparoendosc Adv Surg Tech A 32(7):768–774. https://doi.org/10.1089/lap.2021.0150
Stefanidis D, Wang F, Korndorffer JR, Dunne JB, Scott DJ (2010) Robotic assistance improves intracorporeal suturing performance and safety in the operating room while decreasing operator workload. Surg Endosc 24(2):377–382. https://doi.org/10.1007/s00464-009-0578-0
Sharma G, Strong AT, Tu C, Brethauer SA, Schauer PR, Aminian A (2018) Robotic platform for gastric bypass is associated with more resource utilization: an analysis of MBSAQIP dataset. Surg Obes Relat Dis 14(3):304–310. https://doi.org/10.1016/j.soard.2017.11.018
Funding
Support for the Michigan Bariatric Surgery Collaborative (MBSC) is provided by Blue Cross and Blue Shield of Michigan and Blue Care Network as part of the BCBSM Value Partnerships program.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Jonathan Finks and Amir Ghaferi receive salary support from Blue Cross Blue Shield of Michigan for leadership and participation in the Michigan Bariatric Surgery Collaborative. Drs. Arthur Carlin and Oliver Varban receive an honorarium for their leadership and participation in the Michigan Bariatric Surgery Collaborative. Dr. Anne Ehlers receives unrelated funding from SAGES and the Association for Academic Surgery. Although Blue Cross Blue Shield of Michigan and the Michigan Bariatric Surgery Collaborative (MBSC) work collaboratively, the opinions, beliefs and viewpoints expressed by the author do not necessarily reflect the opinions, beliefs and viewpoints of BCBSM or any of its employees. Ahmad M. Hider, Hollis Johanson, Aaron J. Bonham, Amir A. Ghaferi, Jonathan Finks, Anne P. Ehlers, Arthur M. Carlin and Oliver A. Varban have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Hider, A.M., Johanson, H., Bonham, A.J. et al. Evaluating outcomes among surgeons who changed their technique for gastric bypass: a state-wide analysis from 2011 to 2021. Surg Endosc 37, 8464–8472 (2023). https://doi.org/10.1007/s00464-023-10434-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10434-x