
Abstract
Introduction
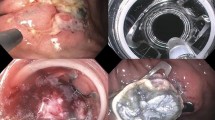
Mucosal lesions located at the ileocecal valve may be challenging for endoscopic intervention because of angulated anatomy and a thinner wall with narrower lumen when compared to other locations of the bowel. This study aimed to evaluate the management and outcomes of ileocecal valve lesions treated endoscopically.
Material and methods
Patients with mucosal neoplasms involving the ileocecal valve managed with advanced endoscopy at a quaternary care hospital between 2011 and 2021 were included from a prospectively collected database. Patient demographics, lesion characteristics, complications, and outcomes are reported.
Results
From 1005 lesions, 80 patients (8%) underwent resection for neoplasms involving ileocecal valve by ESD (n = 38), hybrid ESD (n = 38), EMR (n = 2), and CELS (n = 2). The median age of the study group was 63(37–84) years, and 50% of patients were female. The median lesion size was 34 mm (5–75). The mean procedure time was 66 ± 44 min(range:18–200). The dissection was completed as piecemeal in 41(51%) patients and 35(44%) had en-bloc dissection. Seven(8%) endoscopic interventions required conversion to laparoscopic surgery due to inability to lift the mucosa(n = 4) and perforation(n = 3). No immediate bleeding occurred in the study group. Five patients had late rectal bleeding and two were admitted with post-polypectomy pain within 30 days of intervention. Pathology revealed 4(5%) adenocarcinomas, 33(41.2%) tubular adenomas, 30(37.8%) tubulovillous adenomas, and 5(6.2%) sessile serrated adenomas. Sixty-seven (84.5%) patients completed at least one follow-up colonoscopy and were followed for a median of 11(0–64) months. Six (8.9%) patients had recurrence and were managed with subsequent endoscopic removal.
Conclusion
Advanced endoscopy can be safely and effectively performed for the management of ileocecal valve polyps with low complication and acceptable recurrence rates. Advanced endoscopy promises an alternative approach to oncologic ileocecal resection while attaining organ preservation. Our study demonstrates the impact of advanced endoscopy for the treatment of mucosal neoplasms involving ileocecal valve.




Similar content being viewed by others


References
Ozgur I, Liska D, Cengiz TB, Sapci I, Valente MA, Holubar SD, Steele SR, Bhatt A, Gorgun E (2022) Colectomy for polyps is associated with high risk for complications and low risk for malignancy: Time for endoluminal surgery? Am J Surg 223:463–467
Law R, Das A, Gregory D, Komanduri S, Muthusamy R, Rastogi A, Vargo J, Wallace MB, Raju GS, Mounzer R, Klapman J, Shah J, Watson R, Wilson R, Edmundowicz SA, Wani S (2016) Endoscopic resection is cost-effective compared with laparoscopic resection in the management of complex colon polyps: an economic analysis. Gastrointest Endosc 83:1248–1257
Nanda KS, Tutticci N, Burgess NG, Sonson R, Williams SJ, Bourke MJ (2015) Endoscopic mucosal resection of laterally spreading lesions involving the ileocecal valve: technique, risk factors for failure, and outcomes. Endoscopy 47:710–718
Ishii N, Itoh T, Horiki N, Matsuda M, Setoyama T, Suzuki S, Uemura M, Iizuka Y, Fukuda K, Suzuki K, Fujita Y (2010) Endoscopic submucosal dissection with a combination of small-caliber-tip transparent hood and flex knife for large superficial colorectal neoplasias including ileocecal lesions. Surg Endosc 24:1941–1947
Yoshizaki T, Toyonaga T, Tanaka S, Ohara Y, Kawara F, Baba S, Tsubouchi E, Takihara H, Watanabe D, Ishida T, Hoshi N, Morita Y, Umegaki E, Azuma T (2016) Feasibility and safety of endoscopic submucosal dissection for lesions involving the ileocecal valve. Endoscopy 48:639–645
Gorgun E, Benlice C, Abbas MA, Steele S (2018) Experience in colon sparing surgery in North America: advanced endoscopic approaches for complex colorectal lesions. Surg Endosc 32:3114–3121
Draganov PV, Aihara H, Karasik MS, Ngamruengphong S, Aadam AA, Othman MO, Sharma N, Grimm IS, Rostom A, Elmunzer BJ, Jawaid SA, Westerveld D, Perbtani YB, Hoffman BJ, Schlachterman A, Siegel A, Coman RM, Wang AY, Yang D (2021) Endoscopic submucosal dissection in North America: A large prospective multicenter study. Gastroenterology 160:2317-2327.e2
Ma C, Teriaky A, Sheh S, Forbes N, Heitman SJ, Jue TL, Munroe CA, Jairath V, Corley DA, Lee JK (2019) Morbidity and mortality after surgery for nonmalignant colorectal polyps: A 10-year nationwide analysis. Am J Gastroenterol 114:1802–1810
Peery AF, Shaheen NJ, Cools KS, Baron TH, Koruda M, Galanko JA, Grimm IS (2018) Morbidity and mortality after surgery for nonmalignant colorectal polyps. Gastrointest Endosc 87:243–250
Gorgun E, Benlice C, Church JM (2016) Does cancer risk in colonic polyps unsuitable for polypectomy support the need for advanced endoscopic resections? J Am Coll Surg 223:478–484
Jelbert A, Swinson S, Atkin K, Bhalerao S, Babu S (2008) Imaging of the ileocaecal valve. Tech Coloproctol 12:87–92
Gurram KC, Ly E, Zhang X, Modayil R, Das K, Ramai D, Nithyanand S, Bhumi S, Neppala S, Boinpally H, Stavropoulos S (2020) A novel technique of endoscopic submucosal dissection for circumferential ileocecal valve adenomas with terminal ileum involvement: the “doughnut resection” (with videos). Surg Endosc 34:1417–1424
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Emre Gorgun is consultant for DiLumen, Olympus, and Boston Scientific. Drs. Ilker Ozgur, Carla F. Justiniano, Michael A. Valente, Stefan D. Holubar, Scott R. Steele have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ozgur, I., Justiniano, C.F., Valente, M.A. et al. Are large ileocecal valve lesions amenable with advanced endoscopic management to avoid bowel resection?. Surg Endosc 37, 5320–5325 (2023). https://doi.org/10.1007/s00464-023-10014-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-023-10014-z