
Abstract
Purpose
One of the procedures that has become very popular thanks to the advantages of minimally invasive approach is the laparoscopic treatment of inguinocrural hernias. As a disadvantage, it would imply a longer learning curve when compared to the conventional approach. There is no consensus about the number of procedures required to dominate this surgical technique, since according to bibliography it ranges from 20 to 240.
Methods
We analyzed and compared the progress of 18 third year surgical residents while they were introducing into laparoscopic transabdominal preperitoneal inguinal hernioplasties between June 2013 and May 2018.
Results
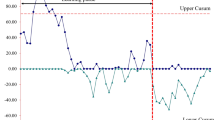
Between June 2013 and May 2018, 1282 laparoscopic inguinal hernioplasties were performed (71 procedures per resident). Mean surgical time was for unilateral: 62.13 min (SD ± 15.54; range 30–105 min) for the first third (Q1) vs 54.61 min (SD ± 15.38; range 30–100 min) for the last third (Q3): p < 0.0001. For bilateral were: 92.59 min (SD ± 21.89; range 50–160 min) for Q1 vs 84.48 min (SD ± 20.52; range 30–130 min) for Q3: p < 0.05. Accepting an alpha error of 5% and considering an association power of 80%, there would be needed 61 cases per surgeon to achieve a significant reduction in surgical time.
Conclusion
In a center with high-volume in TAPP and under a supervised training program, it is feasible to achieve a reduction in surgical time. Randomized studies with a larger number of cases are necessary to confirm this finding and draw more robust and objective conclusions.





Similar content being viewed by others


References
Köckerling F, Sheen AJ, Berrevoet F et al (2019) Accreditation and certification requirements for hernia centers and surgeons: the ACCESS project. Hernia 23(2):185–203. https://doi.org/10.1007/s10029-018-1873-2
Simons MP, Smietanski M, Bonjer HJ et al (2018) International guidelines for groin hernia management. Hernia 22(1):1–65. https://doi.org/10.1007/s10029-017-1668-x
McCormack K, Scott N, Go PMNY, Ross SJ, Grant A (2003) Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.cd001785
Simons MP, Aufenacker T, Bay-Nielsen M et al (2009) European hernia society guidelines on the treatment of inguinal hernia in adult patients. Hernia 13(4):343–403. https://doi.org/10.1007/s10029-009-0529-7
Scheuermann U, Niebisch S, Lyros O, Jansen-Winkeln B, Gockel I (2017) Transabdominal preperitoneal (TAPP) versus Lichtenstein operation for primary inguinal hernia repair—a systematic review and meta-analysis of randomized controlled trials. BMC Surg 17(1):1–10. https://doi.org/10.1186/s12893-017-0253-7
Koju R, Koju RB, Malla B, Dongol Y, Thapa LB (2017) Transabdominal pre-peritoneal mesh repair versus Lichtenstein’s hernioplasty. J Nepal Health Res Counc 15(2):135–140. https://doi.org/10.3126/jnhrc.v15i2.18202
Haidenberg J, Kendrick ML, Meile T, Farley DR (2003) Totally extraperitoneal (TEP) approach for inguinal hernia: the favorable learning curve for trainees. Curr Surg 60(1):65–68. https://doi.org/10.1016/S0149-7944(02)00657-8
Voitk AJ (1998) The learning curve in laparoscopic inguinal hernia repair for the community general surgeon. Can J Surg 41(6):446–450
Bittner R, Schmedt CG, Schwarz J, Kraft K, Leibl BJ (2002) Laparoscopic transperitoneal procedure for routine repair of groin hernia. Br J Surg 89(8):1062–1066. https://doi.org/10.1046/j.1365-2168.2002.02178.x
Choi YY, Kim Z, Hur KY (2012) Learning curve for laparoscopic totally extraperitoneal repair of inguinal hernia. Can J Surg 55(1):33–36. https://doi.org/10.1503/cjs.019610
Giddings HL, Fenton-lee D (2021) Australian general surgical trainee experience with inguinal hernia learning curve. ANZ J Surg. https://doi.org/10.1111/ans.16897
Bracale U, Merola G, Sciuto A, Cavallaro G, Andreuccetti J, Pignata G (2019) Achieving the learning curve in laparoscopic inguinal hernia repair by tapp: a quality improvement study. J Investig Surg 32(8):738–745. https://doi.org/10.1080/08941939.2018.1468944
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213. https://doi.org/10.1097/01.sla.0000133083.54934.ae
Clavien PA, Barkun J, De Oliveira ML et al (2009) The clavien-dindo classification of surgical complications: five-year experience. Ann Surg 250(2):187–196. https://doi.org/10.1097/SLA.0b013e3181b13ca2
Hasbahceci M, Basak F, Acar A, Alimoglu O (2014) “A new proposal for learning curve of TEP Inguinal hernia repair: ability to complete operation endoscopically as a first phase of learning curve.” Minim Invasive Surg 528517:5. https://doi.org/10.1155/2014/528517
The HerniaSurge Group (2018) International guidelines for groin hernia management. Hernia 22:1–165. https://doi.org/10.1007/s10029-017-1668-x
Bökeler U, Schwarz J, Bittner R, Zacheja S, Smaxwil C (2013) Teaching and training in laparoscopic inguinal hernia repair (TAPP): impact of the learning curve on patient outcome. Surg Endosc 27(8):2886–2893. https://doi.org/10.1007/s00464-013-2849-z
Funding
No source of funding.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by JFA, LM, FO, PM, DB, EAP and DEP. The first draft of the manuscript was written by JFA and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Disclosures
Drs. Joaquin Fernandez-Alberti, Lautaro Mata, Facundo Orrego, Pablo Medina, Diego Bogetti, Eduardo Agustin Porto and Daniel Enrique Pirchi have no conflicts of interest or financial ties to disclose. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical approval
Ethical approval was waived by the local Ethics Committee of the British Hospital of Buenos Aires in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Consent to participate
Due to the retrospective nature of the study, the Ethics Committee waived the requirement for written informed consent; however, all patients signed the surgical consent form.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fernandez-Alberti, J., Mata, L., Orrego, F. et al. Laparoscopic inguinal hernia repair: impact of surgical time in the learning curve. Surg Endosc 37, 2826–2832 (2023). https://doi.org/10.1007/s00464-022-09807-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09807-5