
Abstract
Introduction
Use of robotic-assisted surgery is increasing, and resident involvement may lead to higher costs. We investigated whether senior resident involvement in noncomplex robotic cholecystectomy (RC) and inguinal hernia (RIH) would take more time and cost more when compared to non-robotic cholecystectomy (NRC) and inguinal hernia repair (NRIH).
Methods
We extracted surgery duration and total cost of NRC, NRIH, RC, and RIH from 7/2016 to 6/2020 with senior resident (PGY4-5) involvement. We excluded complex cases as well as prisoner cases and those with new faculty and research residents. We assessed differences between robotic and non-robotic cases in surgery duration and total cost per minute, using one-way ANOVA.
Results
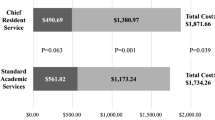
We included 1608 cases (non-robotic 1145 vs. robotic 463). On average, RC cases with a senior resident took less time than NRC (179.4 < 185.8, p = 0.401); surgery duration of RIH cases was similar with NRIH cases. The total cost per minute of RC cases with a senior resident on average was $9.30 higher than NRC cases for each minute incurred in the operating room but did not lead to a significant change in overall cost. RIH cases, on the other hand, cost less per minute than NRIH cases (114.1 < 126.5, p = 0.399).
Conclusion
Training in robotic surgery is important. Noncomplex RC and RIH involving senior residents were not significantly longer nor did they incur significantly more cost than non-robotic procedures. Senior resident training in noncomplex robotic surgery can be efficient and can be included in the residency curriculum.
Graphical abstract


Similar content being viewed by others


References
Armijo PR, Pagkratis S, Boilesen E, Tanner T, Oleynikov D (2017) Growth in robotic-assisted procedures is from conversion of laparoscopic procedures and not from open surgeons’ conversion: a study of trends and costs. Surg Endosc 32:2106–2113
Dulan G, Rege RV, Hogg DC, Gilberg-Fisher KM, Arain NA, Tesfay ST, Scott DJ (2012) Developing a comprehensive, proficiency-based training program for robotic surgery. Surgery 152(3):477–488. https://doi.org/10.1016/j.surg.2012.07.028
Vetter MH, Palettas M, Hade E, Fowler J, Salani R (2018) Time to consider integration of a formal robotic-assisted surgical training program into obstetrics/gynecology residency curricula. J Robot Surg 12(3):517–521. https://doi.org/10.1007/s11701-017-0775-0
Zhao B, Lam J, Hollandsworth HM, Lee AM, Lopez NE, Abbadessa B, Eisenstein S, Cosman BC, Ramamoorthy SL, Parry LA (2020) General surgery training in the era of robotic surgery: a qualitative analysis of perceptions from resident and attending surgeons. Surg Endosc 34(4):1712–1721. https://doi.org/10.1007/s00464-019-06954-0
Simianu VV, Gaertner WB, Kuntz K, Kwaan MR, Lowry AC, Madoff RD, Jensen CC (2020) Cost-effectiveness evaluation of laparoscopic versus robotic minimally invasive colectomy. Ann Surg 272(2):334–341. https://doi.org/10.1097/SLA.0000000000003196
Ferri V, Quijano Y, Nuñez J, Caruso R, Duran H, Diaz E, Fabra I, Malave L, Isernia R, d’Ovidio A, Agresott R, Gomez P, Isojo R, Vicente E (2021) Robotic-assisted right colectomy versus laparoscopic approach: case-matched study and cost-effectiveness analysis. J Robot Surg 15(1):115–123. https://doi.org/10.1007/s11701-020-01084-5
Khorgami Z, Li WT, Jackson TN, Howard CA, Sclabas GM (2019) The cost of robotics: an analysis of the added costs of robotic-assisted versus laparoscopic surgery using the national inpatient sample. Surg Endosc 33(7):2217–2221. https://doi.org/10.1007/s00464-018-6507-3
Ye L, Childers CP, de Virgilio M, Shenoy R, Mederos MA, Mak SS, Begashaw MM, Booth MS, Shekelle PG, Wilson M, Gunnar W, Girgis MD, Maggard-Gibbons M (2021) Clinical outcomes and cost of robotic ventral hernia repair: systematic review. BJS Open. 5(6):zrab098. https://doi.org/10.1093/bjsopen/zrab098
Merola G, Sciuto A, Pirozzi F, Andreuccetti J, Pignata G, Corcione F, Milone M, De Palma GD, Castaldo R, Pecchia L, Ceccarelli G, Bracale U (2020) Is robotic right colectomy economically sustainable? A multicentre retrospective comparative study and cost analysis. Surg Endosc 34(9):4041–4047. https://doi.org/10.1007/s00464-019-07193-z
Chen XP, Cochran A, Harzman A, Ellison EC (2020) A novel operative coaching program for general surgery chief residents improves operative efficiency. J Surg Educ S1931–7204(20):30474–30478. https://doi.org/10.1016/j.jsurg.2020.12.006
Davis SS Jr, Husain FA, Lin E, Nandipati KC, Perez S, Sweeney JF (2013) Resident participation in index laparoscopic general surgical cases: impact of the learning environment on surgical outcomes. J Am Coll Surg 216(1):96–104. https://doi.org/10.1016/j.jamcollsurg.2012.08.014
Wilkiemeyer M, Pappas TN, Giobbie-Hurder A, Itani KM, Jonasson O, Neumayer LA (2005) Does resident post graduate year influence the outcomes of inguinal hernia repair? Ann Surg 241(6):879–882. https://doi.org/10.1097/01.sla.0000164076.82559.72
Kasotakis G, Doherty G (2015) Trainee participation in emergency surgery: what are the consequences? Adv Surg 49:131–141. https://doi.org/10.1016/j.yasu.2015.04.001
Childers CP, Maggard-Gibbons M (2018) Understanding costs of care in the operating room. JAMA Surg 153(4):e176233. https://doi.org/10.1001/jamasurg.2017.6233
Chen XP, Sullivan AM, Smink DS, Alseidi A et al (2019) Resident autonomy in the operating room: how faculty assess real-time entrustability. Ann Surg 269(6):1080–1086. https://doi.org/10.1097/SLA.0000000000002717
Chen XP, Sullivan AM, Bengtson JM, Dalrymple JL (2017) Entrustment evidence used by expert gynecologic surgical teachers to determine residents’ autonomy. Obstet Gynecol 130(Suppl 1):8S-16S
Torbeck L, Wilson A, Choi J, Dunningham GL (2015) Identification of behaviors and techniques for promoting autonomy in the operating room. Surgery 158(4):112–210
Sugiyama T, Liew SL (2017) The effects of sensory manipulations on motor behavior: from basic science to clinical rehabilitation. J Mot Behav 49(1):67–77. https://doi.org/10.1080/00222895.2016.1241740
Funding
This project was supported by Award Number UL1TR002733 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Xiaodong (Phoenix) Chen receives grants from AMA and Intuitive Foundation and is on the Editorial Board of Global Surgical Education—Journal of the Association for Surgical Education. Dr. Ellison receives royalties from McGraw Hill and Wolters Kluwer and is the ACS President and on the ASA Council and Foundation Board. Dr. Meara receives a grant and honoraria from Intuitive Foundation. Dr. Harzman and Ms. Pieper have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chen, X., Meara, M., Harzman, A. et al. Cost analysis of training residents in robotic-assisted surgery. Surg Endosc 37, 2765–2769 (2023). https://doi.org/10.1007/s00464-022-09794-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09794-7