
Abstract
Background and aims
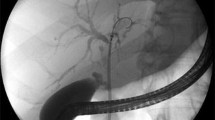
There are limited data about the benign biliary strictures (BBS) which can develop during the clinical course of acute biliary pancreatitis (ABP) due to compression of the common bile duct (CBD) by edematous and inflamed pancreatic tissue. We aimed to determine the incidence of BBS due to ABP and its clinical course after endoscopic management.
Methods
The study was retrospectively conducted among patients with ABP who were admitted to a single tertiary reference center during 3 years. BBS-ABP was defined as distal narrowing of the CBD with proximal dilatation and delayed drainage of the contrast into the duodenum. Endoscopic treatment was performed by inserting a single 7F or 10F plastic stent which was exchanged every 3 months until stricture resolution. Patients were followed for 1 year after stricture resolution.
Results
Seven hundred and twenty-one patients had ABP during the study period. Among them, 257 (35.6%) patients underwent ERCP and 26 patients (3.6%) had CBD stricture due to ABP. A 7 Fr plastic stent was inserted in 18 patients and 10 Fr in 8 patients. The stricture was completely resolved at 3 months in 66.7%, at 6 months 23.8% and at 9 months (9.5%) of the patients. There was no procedure-related complications other than asymptomatic stent migration in 4 (19%) patients. None of the patients had recurrent biliary stricture during the 1 year stent-free follow-up period.
Conclusion
BBS-ABP is a frequently seen clinical entity. In most patients, the stricture improves within 3 months and temporary endoscopic stenting prevents the patients from the consequences of the obstruction during this period.




Similar content being viewed by others


Abbreviations
- ABP:
-
Acute biliary pancreatitis
- AIP:
-
Autoimmune pancreatitis
- ARFI:
-
Acoustic Radiation Force Impulse
- BBS-ABP:
-
Benign biliary strictures associated with acute biliary pancreatitis,
- CBD:
-
Common bile duct
- CP:
-
Chronic pancreatitis
- CT:
-
Computed tomography
- ERCP:
-
Endoscopic retrograde cholangiopancreatography
- EUS:
-
Endoscopic ultrasonography
- FC-SEMS:
-
Fully covered self-expandable metal stent
- MRCP:
-
Magnetic resonance cholangiopancreatography
- PP:
-
Pancreatic pseudocyst
- PTC:
-
Percutaneous transhepatic cholangiography
- SWV:
-
Shear wave velocity
- SPSS:
-
Statistical Package for Social Sciences
- WON:
-
Walled-off necrosis
References
Rodrigues T, Boike JR (2021) Biliary strictures: etiologies and medical management. Semin Intervent Radiol 38(3):255–262
Hollinghead W (1957) The lower part of the common bile duct, a review. Surg Clin North Am 37:939–952
Buxbaum J (2012) The role of endoscopic retrograde cholangiopancreatography in patients with pancreatic disease. Gastroenterol Clin North Am 41(1):23–45
Riff BP, Chandrasekhara V (2016) The role of endoscopic retrograde cholangiopancreatography in management of pancreatic diseases. Gastroenterol Clin North Am 45(1):45–65
Frieden JH (1965) The significance of jaundice in acute pancreatıtıs. Arch Surg 90:422–426
Kuo VC, Tarnasky PR (2013) Endoscopic management of acute biliary pancreatitis. Gastrointest Endosc Clin N Am 23(4):749–768
Easler JJ, Sherman S (2015) Endoscopic retrograde cholangiopancreatography for the management of common bile duct stones and gallstone pancreatitis. Gastrointest Endosc Clin N Am 25(4):657–775
Banks PA, Bollen TL, Dervenis C et al (2013) Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut 62(1):102–111
Yu W, Li W, Wang Z, Ye X, Li N, Li J (2007) Early percutaneous transhepatic gallbladder drainage compared with endoscopic retrograde cholangiopancreatography and papillotomy treatment for severe gallstone associated acute pancreatitis. Postgrad Med J 83(977):187–191
Tenner S, Dubner H, Steinberg W (1984) Predicting gallstone pancreatitis with laboratory parameters: a meta-analysis. Am J Gastroenterol 89:1863–1866
Roberts SE, Morrison-Rees S, John A, Williams JG, Brown TH, Samuel DG (2017) The incidence and aetiology of acute pancreatitis across Europe. Pancreatology 17(2):155–165
Vitale GC, Reed DN Jr, Nguyen CT, Lawhon JC, Larson GM (2000) Endoscopic treatment of distal bile duct stricture from chronic pancreatitis. Surg Endosc 14(3):227–231
Draganov P, Hoffman B, Marsh W, Cotton P, Cunningham J (2002) Long-term outcome in patients with benign biliary strictures treated endoscopically with multiple stents. Gastrointest Endosc 55:680–686
Cotton PB, Lehman G, Vennes J, et al. (1991) Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 37(3):383–393
Skandalakis LJ, Skandalakis JE (2014) Surgical Anatomy and Technique, A Pocket Manual, 4th edn. Springer, New York, USA
Eckhauser FE, Knol JA, Strodel WE, Achem S, Nostrant T (1983) Common bile duct strictures associated with chronic pancreatitis. Am Surg 49(7):350–358
Almadi MA, Barkun JS, Barkun AN (2015) Stenting in malignant biliary obstruction. Gastrointest Endosc Clin N Am 25(4):691–711
Bill JG, Mullady DK (2019) Stenting for benign and malignant biliary strictures. Gastrointest Endosc Clin N Am 29(2):215–235
Madhani K, Farrell JJ (2018) Management of autoimmune pancreatitis. Gastrointest Endosc Clin N Am 28(4):493–519
Baron TH, DiMaio CJ, Wang AY, Morgan KA (2020) American gastroenterological association clinical practice update: management of pancreatic necrosis. Gastroenterology 158(1):67–75
Coutinho LMA, Bernardo WM, Rocha RS et al (2018) Early endoscopic retrograde cholangiopancreatography versus conservative treatment in patients with acute biliary pancreatitis: systematic review and meta-analysis of randomized controlled trials. Pancreas 47(4):444–453
Familiari P, Boškoski I, Bove V, Costamagna G (2013) ERCP for biliary strictures associated with chronic pancreatitis. Gastrointest Endosc Clin N Am 23(4):833–845
Xie J, Zou L, Yao M, Xu G, Zhao L, Xu H, Wu R (2015) A preliminary investigation of normal pancreas and acute pancreatitis elasticity using virtual touch tissue quantification (VTQ) imaging. Med Sci Monit 11(21):1693–1699
Yashima Y, Sasahira N, Isayama H et al (2012) Acoustic radiation force impulse elastography for noninvasive assessment of chronic pancreatitis. J Gastroenterol 47(4):427–432
Săftoiu A, Vilmann P, Gorunescu F et al (2008) Neural network analysis of dynamic sequences of EUS elastography used for the differential diagnosis of chronic pancreatitis and pancreatic cancer. Gastrointest Endosc 68(6):1086–1094
Hirooka Y, Kuwahara T, Irisawa A et al (2015) JSUM ultrasound elastography practice guidelines: pancreas. J Med Ultrason 42(2):151–174
Ishikawa T, Kawashima H, Ohno E et al (2020) Usefulness of endoscopic ultrasound elastography combined with the strain ratio in the estimation of treatment effect in autoimmune pancreatitis. Pancreas 49(2):e21–e22
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr Ahmet Tarık Eminler, Dr Aydin Seref Koksal, Dr Bilal Toka, Dr Cengiz Karacaer, Dr Mustafa Ihsan Uslan, and Dr Erkan Parlak have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Eminler, A.T., Koksal, A.S., Toka, B. et al. Benign biliary strictures associated with acute biliary pancreatitis. Surg Endosc 37, 2587–2594 (2023). https://doi.org/10.1007/s00464-022-09753-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09753-2