
Abstract
Background
Cervical anastomotic strictures after esophagectomy cause significant disease burden. We aimed to study the technical feasibility and safety of intensive endoscopic therapy.
Methods
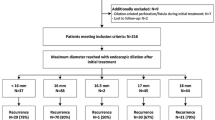
In this pilot study, we included 15 patients with an untreated benign cervical anastomotic stricture after esophagectomy. Intensive endoscopic therapy comprised three endoscopic modalities: in- and excision using a needle-knife, intralesional steroid injections and bougie dilation. In two endoscopic procedures, the stricture was dilated up to a luminal diameter of 18 mm. Patients were followed up to 6 months.
Results
A luminal diameter of 18 mm was achieved in 13 of 15 patients (87%) after two endoscopic procedures. No major adverse events related to the investigational treatment occurred. Median dysphagia scores significantly improved from 2 (IQR, interquartile range, 2–3) at baseline to 0 (IQR 0–1) after 14 days (p < 0.001). Eleven (73%) patients developed recurrent symptoms of dysphagia requiring a median of 1 (IQR 0–3) additional endoscopic dilation procedure.
Conclusions
Achieving a luminal diameter of 18 mm in two procedures with intensive endoscopic therapy was technically feasible and effective in reducing dysphagia rapidly in patients with a cervical anastomotic stricture after esophagectomy. No major adverse events related to the investigational treatment were observed.


Similar content being viewed by others

References
van Workum F, van der Maas J, van den Wildenberg FJ, Polat F, Kouwenhoven EA, van Det MJ, Nieuwenhuijzen GA, Luyer MD, Rosman C (2017) Improved functional results after minimally invasive esophagectomy: intrathoracic versus cervical anastomosis. Ann Thorac Surg 103(1):267–273. https://doi.org/10.1016/j.athoracsur.2016.07.010
Huang Q, Zhong J, Yang T, Li J, Luo K, Zheng Y, Yang H, Fu J (2015) Impacts of anastomotic complications on the health-related quality of life after esophagectomy. J Surg Oncol 111(4):365–370. https://doi.org/10.1002/jso.23837
van Halsema EE (2018) Endoscopic treatment of stenoses and leaks in the gastrointestinal tract: the role of self-expandable metal stents. Part I: benign esophageal strictures and leaks. PhD thesis, Digital Academic Repository of the University of Amsterdam (UvA-DARE). https://dare.uva.nl/
Hordijk ML, van Hooft JE, Hansen BE, Fockens P, Kuipers EJ (2009) A randomized comparison of electrocautery incision with Savary bougienage for relief of anastomotic gastroesophageal strictures. Gastrointest Endosc 70(5):849–855. https://doi.org/10.1016/j.gie.2009.02.023
Hirdes MM, van Hooft JE, Koornstra JJ, Timmer R, Leenders M, Weersma RK, Weusten BL, van Hillegersberg R, van Berge Henegouwen MI, Plukker JT, Wiezer R, Bergman JG, Vleggaar FP, Fockens P, Siersema PD (2013) Endoscopic corticosteroid injections do not reduce dysphagia after endoscopic dilation therapy in patients with benign esophagogastric anastomotic strictures. Clin Gastroenterol Hepatol https://doi.org/10.1016/j.cgh.2013.01.016
Hanaoka N, Ishihara R, Motoori M, Takeuchi Y, Uedo N, Matsuura N, Hayashi Y, Yamada T, Yamashina T, Higashino K, Akasaka T, Yano M, Ito Y, Miyata H, Sugimura K, Hamada K, Yamasaki Y, Kanesaka T, Aoi K, Ito T, Iishi H (2018) Endoscopic balloon dilation followed by intralesional steroid injection for anastomotic strictures after esophagectomy: a randomized controlled trial. Am J Gastroenterol 113(10):1468–1474. https://doi.org/10.1038/s41395-018-0253-y
Ogilvie AL, Dronfield MW, Ferguson R, Atkinson M (1982) Palliative intubation of oesophagogastric neoplasms at fibreoptic endoscopy. Gut 23(12):1060–1067
van Halsema EE, Noordzij IC, van Berge Henegouwen MI, Fockens P, Bergman JJ, van Hooft JE (2017) Endoscopic dilation of benign esophageal anastomotic strictures over 16 mm has a longer lasting effect. Surg Endosc 31(4):1871–1881. https://doi.org/10.1007/s00464-016-5187-0
Park JY, Song HY, Kim JH, Park JH, Na HK, Kim YH, Park SI (2012) Benign anastomotic strictures after esophagectomy: long-term effectiveness of balloon dilation and factors affecting recurrence in 155 patients. AJR 198(5):1208–1213. https://doi.org/10.2214/AJR.11.7608
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Emo E. van Halsema, Jacques J.G.H.M. Bergman, Johanna W. van Sandick, Annemieke Cats, Alexander A.F.A. Veenhof and Jolanda M. van Dieren have no conflicts of interest or financial ties to disclose. Prof. Mark I. van Berge Henegouwen declares grants from Stryker and consultancy for Johnson and Johnson, Alesi Surgical, Mylan, BBraun and Medtronic. All fees and grants paid to institution. Prof. Jeanin E. van Hooft has received research support from Cook Medical and acted as consultant for Cook Medical, Boston Scientific, Olympus, Medtronics and Abbvie.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
van Halsema, E.E., Bergman, J.J.G.H.M., van Sandick, J.W. et al. Intensive endoscopic therapy for untreated cervical anastomotic strictures after esophagectomy: a pilot study. Surg Endosc 37, 2029–2034 (2023). https://doi.org/10.1007/s00464-022-09731-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09731-8