
Abstract
Background
Robotic-assisted general surgery procedures are becoming commonplace, requiring more residency programs to establish training curricula for residents. Concerns exist regarding the impact this will have on surgical residents’ operative case distribution in laparoscopic and open surgery. This study aimed to analyze the impact of a growing robotic operative case volume and established robotic surgery training curriculum on the general surgery resident operative experience.
Methods
The robotic surgery training curriculum at the Medical College of Wisconsin was established in 2017. ACGME operative case logs of residents from 2014 to 2020 were analyzed to determine resident participation in open, laparoscopic, and robotic cases. Case categories included alimentary tract, abdomen, endocrine, thoracic, pediatric, and trauma. A one-way analysis of variance (ANOVA) was used to analyze overall cases, as well as participation by case type, post-graduate year (PGY) level, resident role, and institution type. Statistical significance was defined as a p value < 0.05.
Results
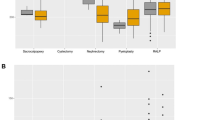
Operative case logs from 77 residents were analyzed with a total of 34,757 cases: 59.3% open, 39.6% laparoscopic, and 1.1% robotic. There was no significant change in open or laparoscopic case volumes. However, there was a 3.4% increase in robotic cases, from 2014 to 2020 (p = 0.01), specifically in foregut (4.0%, p = 0.01), intestinal (1.6%, p = 0.03), and hernia (8.3%, p = 0.003) procedures. Academic (2.8%, p = 0.01) and veterans’ hospital (2.0%, p = 0.01) institutions saw a significant increase in their residents’ robotic cases. The only resident role with a significant increase in robotic cases was first assistant (8.0%, p = 0.004). There was no significant difference across PGY levels by surgical approach.
Conclusions
This study highlights that the growth of robotic cases has not had a detrimental effect on the resident experience with open and laparoscopic cases. As robotic cases continually increase, the impact on laparoscopic and open case volumes must be monitored to ensure a well-balanced training experience.



Similar content being viewed by others


References
Bingmer K, Ofshteyn A, Stein SL, Marks JM, Steinhagen E (2020) Decline of open surgical experience for general surgery residents. Surg Endosc 34(2):967–972. https://doi.org/10.1007/s00464-019-06881-0
Richards MK, McAteer JP, Drake FT, Goldin AB, Khandelwal S, Gow KW (2015) A national review of the frequency of minimally invasive surgery among general surgery residents: assessment of ACGME case logs during 2 decades of general surgery resident training. JAMA Surg 150(2):169–172. https://doi.org/10.1001/jamasurg.2014.1791
Pernar LIM, Robertson FC, Tavakkoli A, Sheu EG, Brooks DC, Smink DS (2017) An appraisal of the learning curve in robotic general surgery. Surg Endosc 31(11):4583–4596. https://doi.org/10.1007/s00464-017-5520-2 (Epub 2017 Apr 14 PMID: 28411345)
Zhao B, Lam J, Hollandsworth HM, Lee AM, Lopez NE, Abbadessa B, Eisenstein S, Cosman BC, Ramamoorthy SL, Parry LA. General surgery training in the era of robotic surgery: a qualitative analysis of perceptions from resident and attending surgeons. Surg Endosc. 2020;34(4):1712–1721. https://doi.org/10.1007/s00464-019-06954-0.
Mehaffey JH, Michaels AD, Mullen MG, Yount KW, Meneveau MO, Smith PW, Friel CM, Schirmer BD (2017) Adoption of robotics in a general surgery residency program: at what cost? J Surg Res 1(213):269–273. https://doi.org/10.1016/j.jss.2017.02.052
Stewart CL, Ituarte PHG, Melstrom KA, Warner SG, Melstrom LG, Lai LL, Fong Y, Woo Y (2019) Robotic surgery trends in general surgical oncology from the National Inpatient Sample. Surg Endosc 33(8):2591–2601. https://doi.org/10.1007/s00464-018-6554-9
Subhas G, Mittal VK (2011) Minimally invasive training during surgical residency. Am Surg 77(7):902–906. https://doi.org/10.1177/000313481107700728
Alkhoury F, Martin JT, Contessa J, Zuckerman R, Nadzam G (2010) The impact of laparoscopy on the volume of open cases in general surgery training. J Surg Educ 67(5):316–319. https://doi.org/10.1016/j.jsurg.2010.08.001
Chung RS, Wojtasik L, Pham Q, Chari V, Chen P (2003) The decline of training in open biliary surgery: effect on the residents’ attitude toward bile duct surgery. Surg Endosc 17(2):338–341. https://doi.org/10.1007/s00464-002-8621-4
Costa AD (2002) Teaching gall bladder surgery: remembrance of things past, or defensive cholecystectomy revisited. ANZ J Surg 69(12):834–836. https://doi.org/10.1046/j.1440-1622.1999.01711.x
Melmer PD, Chaconas C, Taylor R, Verrico E, Cockcroft A, Pinnola A, Holmes S, Sciarretta JD, Davis JM (2019) Impact of laparoscopy on training: are open appendectomy and cholecystectomy on the brink of extinction? Am Surg 85(7):761–763. https://doi.org/10.1177/000313481908500739
Kelly S (2020, January 14). Robotic surgeries surge to 15% of all procedures, despite limited evidence. MedTech Dive. https://www.medtechdive.com/news/robotic-surgeries-surge-to-15-of-all-procedures-despite-limited-evidence/570370/
Sheetz KH, Claflin J, Dimick JB (2020) Trends in the adoption of robotic surgery for common surgical procedures. JAMA Netw Open 3(1):e1918911. https://doi.org/10.1001/jamanetworkopen.2019.18911
Villano AM, Zeymo A, Houlihan BK, Bayasi M, Al-Refaie WB, Chan KS (2019) Minimally invasive surgery for colorectal cancer: hospital type drives utilization and outcomes. J Surg Res. https://doi.org/10.1016/j.jss.2019.07.102
Kadakia N, Malek K, Lee SK, Lee EJ, Burruss S, Srikureja D, Mukherjee K, Lum SS (2020) Impact of robotic surgery on residency training for herniorrhaphy and cholecystectomy. Am Surg 86(10):1318–1323. https://doi.org/10.1177/0003134820964430
Cimen HI, Atik YT, Gul D, Uysal B, Balbay MD (2019) Serving as a bedside surgeon before performing robotic radical prostatectomy improves surgical outcomes. Int Braz J Urol 45(6):1122–1128. https://doi.org/10.1590/S1677-5538.IBJU.2019.0330
Nygaard RM, Daly SR, Van Camp JM (2015) General surgery resident case logs: do they accurately reflect resident experience? J Surg Educ 72(6):e178–e183. https://doi.org/10.1016/j.jsurg.2015.04.022
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Nnenna Nwaelugo has no disclosures to report. Dr. Jon Gould is a consultant for Ethicon, WL Gore, and BD. Dr. Matthew Goldblatt has the following disclosures: Speaking and consulting for W.L. Gore; Speaking, consulting, and research for Medtronic; and Research for Bard. Dr. Rana Higgins is a speaker for WL Gore and Intuitive Surgical.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nwaelugo, N.S., Goldblatt, M.I., Gould, J.C. et al. The evolution of the general surgery resident operative case experience in the era of robotic surgery. Surg Endosc 36, 6679–6687 (2022). https://doi.org/10.1007/s00464-021-08940-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-021-08940-x