
Abstract
Background and aims
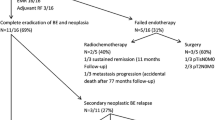
Complete esophageal obstruction (CEO) is a rare complication after radiochemotherapy that dramatically impairs quality of life. Within this study, we assessed the outcome of two different endoscopic techniques for lumen restoration in patients with CEO.
Methods
17 patients were included. Esophageal recanalization was performed in an antegrade approach (Group A) or through combined antegrade and retrograde recanalization and dilatation (CARD, Group B). Technical success, complications, and dysphagia development during follow-up (FU) were compared between the groups.
Results
In Group A (n = 6), esophageal recanalization was performed by a single endoscopist with a median duration of 47 min. In two patients, antegrade recanalization led to formation of a false lumen (i.e., submucosal tunneling) followed by mediastinitis. In Group B, 21 CARD procedures were performed in 11 patients with a technical success rate of 100%. Procedure time was longer compared to Group A; however, no intra- or postprocedural complications were observed in Group B.
Conclusions
In our experience and cohort, CARD was a successful procedure for recanalization of CEO, which exhibits a more favorable safety profile over antegrade recanalization. Further randomized studies to evaluate the treatment of CEO with CARD are needed.


Similar content being viewed by others

References
Coia LR, Myerson RJ, Tepper JE (1995) Late effects of radiation therapy on the gastrointestinal tract. Int J Radiat Oncol Biol Phys 31:1213–1236
Lee WT, Akst LM, Adelstein DJ, Saxton JP, Wood BG, Strome M, Butler RS, Esclamado RM (2006) Risk factors for hypopharyngeal/upper esophageal stricture formation after concurrent chemoradiation. Head Neck 28:808–812
Laurell G, Kraepelien T, Mavroidis P, Lind BK, Fernberg JO, Beckman M, Lind MG (2003) Stricture of the proximal esophagus in head and neck carcinoma patients after radiotherapy. Cancer 97:1693–1700
Wagh MS, Yang D, Chavalitdhamrong D, Draganov PV (2014) Per-oral endoscopic tunneling for restoration of the esophagus (POETRE). Gastrointest Endosc 80:330
O’Sullivan GC, O’Brien MG (1997) Successful retrograde dilation and oesophageal conservation after failed antegrade management of a reflux stricture. Endoscopy 29:141
van Twisk JJ, Brummer RJ, Manni JJ (1998) Retrograde approach to pharyngo-esophageal obstruction. Gastrointest Endosc 48:296–299
Fusco S, Kratt T, Gani C, Stueker D, Zips D, Malek NP, Goetz M (2018) Rendezvous endoscopic recanalization for complete esophageal obstruction. Surg Endosc 32:4256–4262
Maple JT, Petersen BT, Baron TH, Kasperbauer JL, Wong Kee Song LM, Larson MV (2006) Endoscopic management of radiation-induced complete upper esophageal obstruction with an antegrade–retrograde rendezvous technique. Gastrointest Endosc 64:822–828
Grooteman KV, Wong Kee Song LM, Vleggaar FP, Siersema PD, Baron TH (2014) Functional outcome of patients treated for radiation-induced complete esophageal obstruction after successful endoscopic recanalization (with video). Gastrointest Endosc 80:175–181
Vakil N, Morris AI, Marcon N, Segalin A, Peracchia A, Bethge N, Zuccaro G, Bosco JJ, Jones WF (2001) A prospective, randomized, controlled trial of covered expandable metal stents in the palliation of malignant esophageal obstruction at the gastroesophageal junction. Am J Gastroenterol 96:1791–1796
Banerjee A, Rao KS, Nachiappan M (1989) Intrathoracic oesophageal perforations following bouginage: a protocol for management. Aust NZ J Surg 59:563–566
Bueno R, Swanson SJ, Jaklitsch MT, Lukanich JM, Mentzer SJ, Sugarbaker DJ (2001) Combined antegrade and retrograde dilation: a new endoscopic technique in the management of complex esophageal obstruction. Gastrointest Endosc 54:368–372
Jayaraj M, Mohan BP, Mashiana H, Krishnamoorthi R, Adler DG (2019) Safety and efficacy of combined antegrade and retrograde endoscopic dilation for complete esophageal obstruction: a systematic review and meta-analysis. Ann Gastroenterol 32:361–369
Dellon ES, Cullen NR, Madanick RD, Buckmire RA, Grimm IS, Weissler MC, Couch ME, Shaheen NJ (2010) Outcomes of a combined antegrade and retrograde approach for dilatation of radiation-induced esophageal strictures (with video). Gastrointest Endosc 71:1122–1129
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Francesco Vitali, Andreas Nägel, Lukas Pfeifer, Martin Goetz, Jürgen Siebler, Markus F. Neurath, and Timo Rath have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
(MOV 107433 kb)
Rights and permissions
About this article

Cite this article
Vitali, F., Nägel, A., Pfeifer, L. et al. Endoscopic recanalization of complete esophageal obstruction. Surg Endosc 35, 3184–3188 (2021). https://doi.org/10.1007/s00464-021-08313-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-021-08313-4