
Abstract
Background
Colorectal endoscopic submucosal dissection (ESD) remains demanding due to technical difficulties and high risk of perforation. Most of the reported traction methods are initiated after creating a mucosal flap, which is time consuming. To obtain a good visualization at the mucosal incision stage, we developed the early clip-with-line (ECL) method. This method was started immediately after injection of sodium hyaluronate solution into the submucosal layer. In this study, we evaluated the efficacy and the safety of the ECL method for colorectal ESD.
Methods
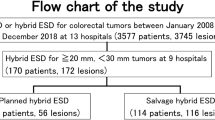
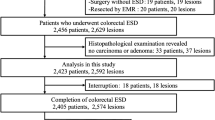
We retrospectively analyzed all cases of colorectal ESDs (41 cases in total) performed from January 2017 to February 2019 in our institution. From January 2017 to August 2018, 27 of these cases were performed using conventional (non-ECL) ESDs, while from September 2018 onwards, the remaining 14 cases were performed using the ECL method. Retrospective comparison between the ECL group and the non-ECL group was conducted in terms of clinical characteristics, treatment outcomes, and adverse events.
Results
There were no significant differences in clinical characteristics between two groups. Procedure time (median [range]) was significantly shorter in the ECL group than in the non-ECL group (66 [29–131] min vs 90 [30–410] min; P = 0.03). As for adverse events, no case of perforation occurred in the ECL group, whereas perforation was observed in 7.4% (2/27) cases in the non-ECL group (no significant difference).
Conclusion
Early clip-with-line method for colorectal endoscopic submucosal dissection reduced procedure time.




Similar content being viewed by others

References
Bray F, Ferlay J, Soerjomataram I et al (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6):394–424
Zauber AG, Winawer SJ, O’Brien MJ et al (2012) Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med 366(8):687–696
Gessl I, Waldmann E, Penz D et al (2019) Evaluation of adenomas per colonoscopy and adenomas per positive participant as new quality parameters in screening colonoscopy. Gastrointest Endosc 89(3):496–502
Rex DK, Schoenfeld PS, Cohen J et al (2015) Quality indicators for colonoscopy. Gastrointest Endosc 81(1):31–53
Hwang JH, Konda V, Abu Dayyeh BK et al (2015) Endoscopic mucosal resection. Gastrointest Endosc 82(2):215–226
Moss A, Williams SJ, Hourigan LF et al (2014) Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut 64(1):57–65
Saito Y, Uraoka T, Yamaguchi Y et al (2010) A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc 72(6):1217–1225
Seo M, Song EM, Cho JW et al (2019) A risk-scoring model for the prediction of delayed bleeding after colorectal endoscopic submucosal dissection. Gastrointest Endosc 89(5):990–998
Lee S, Kim J, Soh JS et al (2018) Recurrence rate of lateral margin-positive cases after en bloc endoscopic submucosal dissection of colorectal neoplasia. Int J Colorectal Dis 33(6):735–743
Ritsuno H, Sakamoto N, Osada T et al (2014) Prospective clinical trial of traction device-assisted endoscopic submucosal dissection of large superficial colorectal tumors using the S-O clip. Surg Endosc 28(11):3143–3149
Yamasaki Y, Takeuchi Y, Uedo N et al (2018) Efficacy of traction-assisted colorectal endoscopic submucosal dissection using a clip-and-thread technique: a prospective randomized study. Dig Endosc 30(4):467–476
Kawaguchi K, Ikebuchi Y, Isomoto H et al (2019) Novel pre-incision clip and traction method for colorectal endoscopic submucosal dissection. Dig Endosc 31(6):e107–e108
Sano Y, Tanaka S, Kudo S et al (2016) Narrow-band imaging (NBI) magnifying endoscopic classification of colorectal tumors proposed by the Japan NBI Expert Team. Dig Endosc 28:526–533
Kudo S, Rubio CA, Teixeira CR et al (2001) Pit pattern in colorectal neoplasia: endoscopic magnifying view. Endoscopy 33:367–373
Xie X, Bai J, Fan C et al (2017) Application of clip traction in endoscopic submucosal dissection to the treatment of early esophageal carcinoma and precancerous lesions. Surg Endosc 31:462–468
Oyama T (2012) Counter traction makes endoscopic submucosal dissection easier. Clin Endosc 45(4):375–378
Yoshida M, Takizawa K, Suzuki S et al (2018) Conventional versus traction-assisted endoscopic submucosal dissection for gastric neoplasms: a multicenter, randomized controlled trial (with video). Gastrointest Endosc 87(5):1231–1240
Kitagawa Y, Suzuki T, Hara T et al (2017) Safety and efficacy of endoscopic submucosal dissection using IT knife nano with clip traction method for early esophageal squamous cell carcinoma. Surg Endosc 32(1):450–455
Koike Y, Hirasawa D, Fujita N et al (2015) Usefulness of the thread-traction method in esophageal endoscopic submucosal dissection: randomized controlled trial. Dig Endosc 27(3):303–309
Yamasaki Y, Takeuchi Y, Hanaoka N et al (2015) A novel traction method using an endoclip attached to a nylon string during colonic endoscopic submucosal dissection. Endoscopy 47(Suppl):1
Suzuki T, Hara T, Kitagawa Y et al (2016) Usefulness of IT knife nano for endoscopic submucosal dissection of large colo-rectal lesions. Acta Gastroenterol Belg 79:186–190
Asayama N, Oka S, Tanaka S et al (2016) Clinical usefulness of a single-use splinting tube for poor endoscope operability in deep colonic endoscopic submucosal dissection. Endosc Int Open 4(6):E614–E617
Hayashi N, Tanaka S, Nishiyama S et al (2014) Predictors of incomplete resection and perforation associated with endoscopic submucosal dissection for colorectal tumors. Gastrointest Endosc 79(3):427–435
Imai K, Hotta K, Yamaguchi Y et al (2017) Endoscopic submucosal dissection for large colorectal neoplasms. Dig Endosc 29(Suppl 2):53–57
Kinoshita S, Nishizawa T, Fujimoto A et al (2020) Complete closure versus simple closure for perforations during colorectal endoscopic submucosal dissection. Endosc Int Open 8(1):E76–E80
Li JW, Ang TL, Wang LM (2019) Endoscopic submucosal dissection of colorectal neoplasms: an audit of its safety and efficacy in a single tertiary centre in Singapore. Singapore Med J 60(10):526–531
Takashiro H, Saito H, Tazawa S et al (2020) Early clip-with-line method for colorectal endoscopic submucosal dissection. Endoscopy. https://doi.org/10.1055/a-1090-7096,Jan29
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Hideyuki Takashiro, Hirofumi Saito, Katsunobu Tawada, Yuhei Oyama, Shinichi Tazawa, Masatoshi Usui, Hiromasa Nomoto, and Kazuhiko Kita have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Video 1: Early clip-with-line method for colorectal endoscopic submucosal dissection. Prior to the procedure, the following preparations are made. First, a long nylon line is inserted into the accessory channel of the scope. The end of the line coming out of the accessory channel is tied to a ZEOCLIP and fixed on the scope with tape. Another end of the line is grasped with light Pean forceps. Next, the scope is inserted. A large (40mm) granular laterally spreading tumor is located in the transverse colon. Hyaluronic acid solution is then injected into the submucosal layer at the anal side of the lesion. The tape fixing the ZEOCLIP is removed, and a ZEOCLIP delivery catheter attaching the ZEOCLIP with line is inserted into the accessory channel. The ZEOCLIP grasp the injected part next to the anal edge of the lesion and the line is pulled gently. A mucosal incision is started from the anal side of the ZEOCLIP. The submucosa to be dissected was widely opened and clearly observed from the beginning to the end of the procedure, and the lesion is easily dissected (wmv 105405 kb)
Rights and permissions
About this article

Cite this article
Takashiro, H., Saito, H., Tawada, K. et al. Efficacy of early clip-with-line method for colorectal endoscopic submucosal dissection. Surg Endosc 36, 321–327 (2022). https://doi.org/10.1007/s00464-020-08280-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-08280-2