
Abstract
Introduction
Esophageal anastomotic stricture is a well-known complication after transhiatal esophagectomy (THE), but there is limited data regarding the initial management and subsequent outcomes after stricture dilation. There is concern that dilating to larger diameters upon the initial encounter, specifically with high-grade strictures, will lead to increased risk for complications. We therefore reviewed one surgeon’s experience with esophageal dilations after THE and provided data and treatment recommendations based upon these findings.
Methods
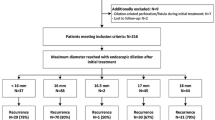
A retrospective review of patients who underwent esophageal dilations ≥ 18 mm up to 20 mm after THE between 2006 and 2019 at our institution was performed. Patient demographics were n = 97, age = 70, 81 males.
Results
For all cases, the mean location, length, diameter of the stricture, and number of days from surgery and initial dilation were 20 cm, 1.9 cm, 6.7 mm, and 106 days, respectively. Most dilations (79%) occurred within 2 weeks to 3 months from surgery. 29.9% were dilated up to 18 mm, 10.3% were dilated up to 19 mm, and 59.8% were dilated up to 20 mm upon initial dilation. Even 1-mm-diameter lesions could be safely dilated upon 18–20 mm. In this study group there were no complications after endoscopic dilation that required hospitalization or further surgical or endoscopic interventions.
Conclusion
These results suggest that early aggressive endoscopic management of esophageal anastomotic strictures after THE can be safely performed.
Similar content being viewed by others


References
Napier KJ, Scheerer M, Misra S (2014) Esophageal cancer: a review of epidemiology, pathogenesis, staging workup and treatment modalities. World J Gastrointest Oncol 6(5):112–120
Park JY, Song HY, Kim JH, Park JH, Na HK, Kim YH, Park SI (2012) Benign anastomotic strictures after esophagectomy: long-term effectiveness of balloon dilation and factors affecting recurrence in 155 patients. AJR Am J Roentgenol 198(5):1208–1213
Egan JV, Baron TH, Adler DG, Davila R, Faigel DO, Gan S-L et al (2006) Esophageal dilation. Gastrointest Endosc 63(6):755–760
Grooteman KV, Wong Kee Song LM, Vleggaar FP, Siersema PD, Baron TH (2017) Non-adherence to the rule of 3 does not increase the risk of adverse events in esophageal dilation. Gastrointest Endosc 85(2):332–337
van Halsema EE, Noordzij IC, van Berge Henegouwen MI, Fockens P, Bergman JJ, van Hooft JE (2017) Endoscopic dilation of benign esophageal anastomotic strictures over 16 mm has a longer lasting effect. Surg Endosc 31(4):1871–1881
Briel JWL, Tamhankar AP, Hagen JA, DeMeester SR, Johansson J, Choustoulakis E, Peters JH, Bremner CG, DeMeester TR (2004) Prevalence and risk factors for ischemia, leak, and stricture of esophageal anastomosis: gastric pull-up versus colon interposition. J Am Coll Surg 198(4):536–541 discussion 541–2
Ahmed Z, Elliott JA, King S, Donohoe CL, Ravi N, Reynolds JV (2017) Risk factors for anastomotic stricture post-esophagectomy with a standardized sutured anastomosis. World J Surg 41:487–497
Lew RJ, Kochman ML (2002) A review of endoscopic methods of esophageal dilation. J Clin Gastroenterol 35(2):117–126
McCain RS, McCain S, Mackle EJ, Tham TCK (2016) Balloon versus bougie for dilatation of benign oesophageal strictures. Cochrane Database Syst Rev 2016(9):CD012343
Pasha SF, Acosta RD, Chandrasekhara V, Chathadi KV, Decker GA, Early DS et al (2014) The role of endoscopy in the evaluation and management of dysphagia. Gastrointest Endosc 79(2):191–201
Langdon DF (1997) The rule of three in esophageal dilation. Gastrointest Endosc 45(1):111
Riley SA, Attwood SE (2004) Guidelines on the use of oesophageal dilatation in clinical practice. Gut 53(Suppl 1):i1–i6
Yoda Y, Yano T, Kaneko K, Tsuruta S, Oono Y, Kojima T et al (2012) Endoscopic balloon dilatation for benign fibrotic strictures after curative nonsurgical treatment for esophageal cancer. Surg Endosc 26:2877–2883
Kim CG, Choi IJ, Lee JY, Cho SJ, Lee JH, Ryu KW et al (2009) Effective diameter of balloon dilation for benign esophagojejunal anastomotic stricture after total gastrectomy. Surg Endosc 23(8):1775–1780
Ben-Menachem T, Decker GA, Early DS, Evans J, Fanelli RD, Fisher DA et al (2012) Adverse events of upper GI endoscopy. Gastrointest Endosc 76(4):707–718
Marjanovic G, Schrag HJ, Fischer E, Hopt UT, Fischer A (2008) Endoscopic bougienage of benign anastomotic strictures in patients after esophageal resection: the effect of the extent of stricture on bougienage results. Dis Esophagus 21(6):551–557
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Jose Martinez and Robert Bowles are consultants and receive research grants from Boston Scientific. Robert Cubas, Robert Andres, Shravan Chintalapani, Estefania Roldan, Andrea Marcadis, and Valerie Wu Chao Ying have no conflict of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cubas, R., Andres, R., Chintalapani, S. et al. Initial management of esophageal anastomotic strictures after transhiatal esophagectomy for esophageal cancer with dilations up to 18–20 mm. Surg Endosc 35, 3488–3491 (2021). https://doi.org/10.1007/s00464-020-07801-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07801-3