
Abstract
Background
Feeding jejunostomy (FJ) is a common treatment to support patients with esophageal cancer after esophagectomy. However, severe FJ-related complications, such as bowel obstruction, occasionally occur. We investigated the ability of our simple, novel FJ technique, the “curtain method,” to prevent bowel obstruction.
Methods
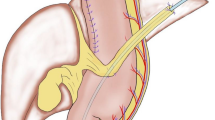
In laparoscopic surgery, the main mechanism of bowel obstruction involves torsion of the mesentery accompanied by migration of the intestine across the fixed FJ through the space surrounded by a triangle comprising the ligament of Treitz, fixed FJ, and spleen rather than adhesion. Our “curtain method” involves closure of this triangle zone with omentum, and the appearance of the lifted omentum resembles a curtain. Sixty patients treated with this modified FJ were retrospectively compared with 13 patients treated with conventional FJ in terms of the incidence of bowel obstruction, peritonitis, stoma site infection, and catheter obstruction.
Results
From 2013 to 2017, 60 patients underwent esophagectomy and gastric conduit reconstruction accompanied by modified laparoscopic FJ. The median observation period, including the period after tube removal, was 644 days. No FJ-associated bowel obstruction, the prevention of which was the primary aim, occurred in any patient. Likewise, no peritonitis or dislodgement occurred. Eight patients (13%) developed a stoma site infection with granulation. The feeding tube became occluded in 11 patients (18%); however, a new feeding tube was reinserted under fluoroscopy for all of these patients. From 2003 to 2012, 13 patients underwent conventional FJ. The median observation period was 387 days. Three patients (23%) developed bowel obstruction by torsion 71 to 134 days after the first surgery, and all were treated by emergency operations. Other FJ-related complications were not different from those in the modified FJ group.
Conclusion
Our simple, novel technique, the “curtain method,” for prevention of laparoscopic FJ-associated bowel obstruction after esophagectomy is a safe additional surgery.



Similar content being viewed by others


References
Berry MF, Atkins BZ, Tong BC, Harpole DH, D’Amico TA, Onaitis MW (2010) A comprehensive evaluation for aspiration after esophagectomy reduces the incidence of postoperative pneumonia. J Thorac Cardiovasc Surg 140:1266–1271
Takeuchi H, Miyata H, Gotoh M, Kitagawa Y, Baba H, Kimura W, Tomita N, Nakagoe T, Shimada M, Sugihara K, Mori M (2014) A risk model for esophagectomy using data of 5354 patients included in a Japanese nationwide web-based database. Ann Surg 260:259–266
Akkerman RD, Haverkamp L, van Rossum PS, van Hillegersberg R, Ruurda JP (2015) Long-term quality of life after oesophagectomy with gastric conduit interposition for cancer. Eur J Cancer 51:1538–1545
Baker M, Halliday V, Williams RN, Bowrey DJ (2016) A systematic review of the nutritional consequences of esophagectomy. Clin Nutr 35:987–994
Sarr MG (1999) Appropriate use, complications and advantages demonstrated in 500 consecutive needle catheter jejunostomies. Br J Surg 86:557–561
Sica GS, Sujendran V, Wheeler J, Soin B, Maynard N (2005) Needle catheter jejunostomy at esophagectomy for cancer. J Surg Oncol 91:276–279
Ryan AM, Rowley SP, Healy LA, Flood PM, Ravi N, Reynolds JV (2006) Post-oesophagectomy early enteral nutrition via a needle catheter jejunostomy: 8-year experience at a specialist unit. Clin Nutr 25:386–393
Mazaki T, Ebisawa K (2008) Enteral versus parenteral nutrition after gastrointestinal surgery: a systematic review and meta-analysis of randomized controlled trials in the English literature. J Gastrointest Surg 12:739–755
Gabor S, Renner H, Matzi V, Ratzenhofer B, Lindenmann J, Sankin O, Pinter H, Maier A, Smolle J, Smolle-Juttner FM (2005) Early enteral feeding compared with parenteral nutrition after oesophageal or oesophagogastric resection and reconstruction. Br J Nutr 93:509–513
Fujita T, Daiko H, Nishimura M (2012) Early enteral nutrition reduces the rate of life-threatening complications after thoracic esophagectomy in patients with esophageal cancer. Eur Surg Res 48:79–84
Takesue T, Takeuchi H, Ogura M, Fukuda K, Nakamura R, Takahashi T, Wada N, Kawakubo H, Kitagawa Y (2015) A prospective randomized trial of enteral nutrition after thoracoscopic esophagectomy for esophageal cancer. Ann Surg Oncol 22:S802–S809
Han-Geurts IJ, Verhoef C, Tilanus HW (2004) Relaparotomy following complications of feeding jejunostomy in esophageal surgery. Dig Surg 21:192–196
Date RS, Clements WD, Gilliland R (2004) Feeding jejunostomy: is there enough evidence to justify its routine use? Dig Surg 21:142–145
Han-Geurts IJ, Hop WC, Verhoef C, Tran KT, Tilanus HW (2007) Randomized clinical trial comparing feeding jejunostomy with nasoduodenal tube placement in patients undergoing oesophagectomy. Br J Surg 94:31–35
Sethuraman SA, Dhar VK, Habib DA, Sussman JE, Ahmad SA, Shah SA, Tsuei BJ, Sussman JJ, Abbott DE (2017) Tube feed necrosis after major gastrointestinal oncologic surgery: institutional lessons and a review of the literature. J Gastrointest Surg 21:2075–2082
Gupta V (2009) Benefits versus risks: a prospective audit. Feeding jejunostomy during esophagectomy. World J Surg 33:1432–1438
Couper G (2011) Jejunostomy after oesophagectomy: a review of evidence and current practice. Proc Nutr Soc 70:316–320
Koterazawa Y, Oshikiri T, Hasegawa H, Yamamoto M, Kanaji S, Yamashita K, Matsuda T, Nakamura T, Suzuki S, Kakeji Y (2019) Routine placement of feeding jejunostomy tube during esophagectomy increases postoperative complications and does not improve postoperative malnutrition. Dis Esophagus [Epub ahead of print]
Fenton JR, Bergeron EJ, Coello M, Welsh RJ, Chmielewski GW (2011) Feeding jejunostomy tubes placed during esophagectomy: are they necessary? Ann Thorac Surg 92(2):504–511
Huang K, Wu B, Ding X, Xu Z, Tang H (2014) Post-esophagectomy tube feeding: a retrospective comparison of jejunostomy and a novel gastrostomy feeding approach. PLoS ONE 9:e89190
Oya H, Koike M, Iwata N, Kobayashi D, Torii K, Niwa Y, Kanda M, Tanaka C, Yamada S, Fujii T, Nakayama G, Sugimoto H, Nomoto S, Fujiwara M, Kodera Y (2015) Feeding duodenostomy decreases the incidence of mechanical obstruction after radical esophageal cancer surgery. World J Surg 39:1105–1110
Young MT, Troung H, Gebhart A, Shih A, Nguyen NT (2016) Outcomes of laparoscopic feeding jejunostomy tube placement in 299 patients. Surg Endosc 30:126–131
Kawai R, Abe T, Uemura N, Fukaya M, Saito T, Komori K, Yokoyama Y, Nagino M, Shinoda M, Shimizu Y (2017) Feeding catheter gastrostomy with the round ligament of the liver prevents mechanical bowel obstruction after esophagectomy. Dis Esophagus 30:1–8
Konishi T, Shiozaki A, Fujiwara H, Konishi H, Takemoto K, Kudou M, Shoda K, Arita T, Kosuga T, Morimura R, Murayama Y, Kuriu Y, Ikoma H, Kubota T, Nakanishi M, Okamoto K, Otsuji E (2018) Comparison of feeding jejunostomy via gastric tube versus jejunum after esophageal cancer surgery. Anticancer Res 38:4941–4945
Ahmed AR, Rickards G, Husain S, Johnson J, Boss T, O’Malley W (2007) Trends in internal hernia incidence after laparoscopic Roux-en-Y gastric bypass. Obes Surg 17(12):1563–1566
Schneider C, Cobb W, Scott J, Carbonell A, Myers K, Bour E (2011) Rapid excess weight loss following laparoscopic gastric bypass leads to increased risk of internal hernia. Surg Endosc 25(5):1594–1598
Toriumi T, Makuuchi R, Kamiya S, Tanizawa Y, Bando E, Terashima M (2019) Obesity is a risk factor for internal hernia after laparoscopic or robot-assisted gastrectomy with mesenteric defect closure for gastric cancer. Surg Endosc Apr 8. [Epub ahead of print]
Llaguna OH, Kim HJ, Deal AM, Calvo BF, Stitzenberg KB, Meyers MO (2011) Utilization and morbidity associated with placement of a feeding jejunostomy at the time of gastroesophageal resection. J Gastrointest Surg 15:1663–1669
Ninomiya I, Makino I, Fujimura T, Fushida S, Oyama K, Kinoshita J, Tajima H, Kitagawa H, Ohta T (2011) Feeding catheter gastrostomy at esophagectomy with gastric tube reconstruction through posterior mediastinal route. Esophagus 8:217–223
Foegeding EA, Bowland EL, Harding CC (1995) Factors that determine the fracture properties and microstructure of globular protein gels. Food Hydrocoll 9:237–249
Acknowledgement
We thank Angela Morben, DVM, ELS, from Edanz Group, for editing a draft of this manuscript.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
SO contributed to the study conception, data acquisition, data interpretation, and writing of the manuscript. YFP contributed to the data acquisition and writing of the manuscript. KH, IM, HY, YA, SM, KY, and IM contributed to the data acquisition. YT contributed to critical revision of the manuscript for important intellectual content. All authors approved the final version of the submitted manuscript and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Disclosures
Osamu Shiraishi, Hiroaki Kato, Mitsuru Iwama, Yoko Hiraki, Atsushi Yasuda, Ying-Feng Peng, Masayuki Shinkai, Yutaka Kimura, Motohiro Imano, and Takushi Yasuda have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shiraishi, O., Kato, H., Iwama, M. et al. A simple, novel laparoscopic feeding jejunostomy technique to prevent bowel obstruction after esophagectomy: the “curtain method”. Surg Endosc 34, 4967–4974 (2020). https://doi.org/10.1007/s00464-019-07289-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07289-6