
Abstract
Background
During bilateral axillo-breast approach (BABA) robotic thyroidectomy (RoT), carbon dioxide (CO2) gas is insufflated into the operative cavity, not only triggering hemodynamic and metabolic changes, but also inducing postoperative pain and gas embolism. Here, we explored whether the new gasless BABA RoT approach was as safe and efficacious as conventional robotic surgery using CO2 insufflation.
Patients and methods
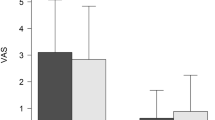
We performed a prospective, randomized controlled trial comparing conventional BABA RoT to gasless BABA RoT (CO2 group, n = 14; gasless group, n = 14). All clinicopathological and oncological outcomes were evaluated. The hemodynamic parameters [heart rate (HR), mean arterial pressure (MAP), cardiac output (CO), and cardiac index (CI)] and metabolic parameters [partial pressure of carbon dioxide (PaCO2) and pH] were measured at baseline; 30, 60, 90, and 120 min after CO2 insufflation; and 30 min after desufflation. Pain parameters [numeric rating scale (NRS) score, number of analgesics (NA), and bottom hit count (BHC)] were measured at 2, 24, 48, and 72 h after surgery.
Results
We found no statistically significant differences between the two groups in terms of any demographic or baseline characteristic. The clinicopathological and oncological outcomes did not differ significantly between the two groups, but the operation time was longer for the gasless group (187.50 ± 42.64 vs. 212.50 ± 35.88 min; P = 0.028). In terms of the hemodynamic, metabolic, and pain parameters, the pH fell significantly less in the gasless group (P = 0.047), but there were no significant between-group differences in the HR, MAP, CO, CI, PaCO2, NRS, NA, or BHC. No safety concerns arose.
Conclusion
The new, gasless BABA RoT technique employing the da Vinci robotic surgical system is safe. Although metabolic changes during operation are thereby minimized, gasless BABA RoT should be used carefully when engaging in thyroid surgery; more experience is required.





Similar content being viewed by others


References
Choi Y, Lee JH, Kim YH, Lee YS, Chang H-S, Park CS, Roh MR (2014) Impact of postthyroidectomy scar on the quality of life of thyroid cancer patients. Ann Dermatol 26:693–699
Lee J, Nah KY, Kim RM, Ahn YH, Soh E-Y, Chung WY (2010) Differences in postoperative outcomes, function, and cosmesis: open versus robotic thyroidectomy. Surg Endosc 24:3186–3194
Linos D (2011) Minimally invasive thyroidectomy: a comprehensive appraisal of existing techniques. Surgery 150:17–24
Miccoli P (2002) Minimally invasive surgery for thyroid and parathyroid diseases. Surg Endosc 16:3–6
Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, Oh SK, Youn YK (2007) Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg 31:601–606
Choi JY, Lee KE, Chung K-W, Kim S-W, Choe J-H, Koo DH, Kim S-j, Lee J, Chung YS, Oh SK (2012) Endoscopic thyroidectomy via bilateral axillo-breast approach (BABA): review of 512 cases in a single institute. Surg Endosc 26:948–955
Lee KE, Rao J, Youn YK (2009) Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: our initial experience. Surg Laparosc Endosc Percutan Tech 19:e71–e75
Lee KE, Kim E, Koo DH, Choi JY, Kim KH, Youn Y-K (2013) Robotic thyroidectomy by bilateral axillo-breast approach: review of 1026 cases and surgical completeness. Surg Endosc 27:2955–2962
Bae DS, Koo DH (2019) A propensity score-matched comparison study of surgical outcomes in patients with pifferentiated thyroid cancer after robotic versus open total thyroidectomy. World J Surg 43:540–551
Kim HY, Choi YJ, Yu HN, Yoon SZ (2012) Optimal carbon dioxide insufflation pressure during robot-assisted thyroidectomy in patients with various benign and malignant thyroid diseases. World J Surg Oncol 10:202
Bellantone R, Lombardi CP, Rubino F, Perilli V, Sollazzi L, Mastroianni G, Gagner M (2001) Arterial PCO2 and cardiovascular function during endoscopic neck surgery with carbon dioxide insufflation. Arch Surg 136:822–827
Hanley ES (1992) Anesthesia for laparoscopic surgery. Surg Clin North Am 72:1013–1019
Holzman M, Sharp K, Richards W (1992) Hypercarbia during carbon dioxide gas insufflation for therapeutic laparoscopy: a note of caution. Surg Laparosc Endosc 2:11–14
Yu W, Li F, Wang Z, Qi X, Li B, Zhang G, Hao X, Hu S (2011) Effects of CO2 insufflation on cerebrum during endoscopic thyroidectomy in a porcine model. Surg Endosc 25:1495–1504
Nyerges A (1994) Pain mechanisms in laparoscopic surgery. Semin Laparosc Surg 1:215–218
Fu J, Luo Y, Chen Q, Lin F, Hong X, Kuang P, Yan W, Wu G, Zhang Y (2018) Transoral endoscopic thyroidectomy: review of 81 cases in a single Institute. J Laparoendosc Adv Surg Tech A 28:286–291
Lee KE, Choi JY, Youn YK (2011) Bilateral axillo-breast approach robotic thyroidectomy. Surg Laparo Endo Per 21:230–236
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L (2016) 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26:1–133
Cho JW, Lee YM, Lee YH, Hong SJ, Yoon JH (2018) Dynamic risk stratification system in post-lobectomy low-risk and intermediate-risk papillary thyroid carcinoma patients. Clin Endocrinol (Oxf) 89:100–109
Button D, Weibel L, Reuthebuch O, Genoni M, Zollinger A, Hofer C (2007) Clinical evaluation of the FloTrac/VigileoTM system and two established continuous cardiac output monitoring devices in patients undergoing cardiac surgery. Br J Anaesth 99:329–336
Lee J, Lee J, Nah K, Soh E, Chung W (2011) Comparison of endoscopic and robotic thyroidectomy. Ann Surg Oncol 18:1439–1446
Bae DS, do Koo H, Choi JY, Kim E, Lee KE, Youn YK (2014) Current status of robotic thyroid surgery in South Korea: a web-based survey. World J Surg 38:2632–2639
Tae K, Lee DW, Song CM, Ji YB, Park JH, Kim DS, Tufano RP (2019) Early experience of transoral thyroidectomy: comparison of robotic and endoscopic procedures. Head Neck 41:730–738
Kim KN, Lee DW, Kim JY, Han KH, Tae K (2018) Carbon dioxide embolism during transoral robotic thyroidectomy: a case report. Head Neck 40:E25–E28
Bae DS, Suh BJ, Park JK, Koo DH (2016) Technical, oncological, and functional safety of bilateral axillo-breast approach (BABA) robotic total thyroidectomy. Surg Laparo Endo Per 26:253–258
Jackson NR, Yao L, Tufano RP, Kandil EH (2014) Safety of robotic thyroidectomy approaches: meta-analysis and systematic review. Head Neck 36:137–143
Gerges FJ, Kanazi GE, Jabbour-Khoury SI (2006) Anesthesia for laparoscopy: a review. J Clin Anesth 18:67–78
Kim JS, Kim KH, Ahn CH, Jeon HM, Kim EG, Jeon CS (2001) A clinical analysis of gasless endoscopic thyroidectomy. Surg Laparosc Endosc Percutan Tech 11:268–272
Campbell MJ, McCoy KL, Shen WT, Carty SE, Lubitz CC, Moalem J, Nehs M, Holm T, Greenblatt DY, Press D (2013) A multi-institutional international study of risk factors for hematoma after thyroidectomy. Surgery 154:1283–1291
Leyre P, Desurmont T, Lacoste L, Odasso C, Bouche G, Beaulieu A, Valagier A, Charalambous C, Gibelin H, Debaene B (2008) Does the risk of compressive hematoma after thyroidectomy authorize 1-day surgery? Langenbeck’s Arch Surg 393:733–737
Acknowledgements
The statistical analysis in the present study was supported by Haeundae Paik Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs Ik Beom Shin, Do Hoon Koo, Myoung Jin Ko, Se Hoon Kim, and Dong Sik Bae have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shin, I.B., Koo, D.H., Ko, M.J. et al. A prospective, randomized controlled study of the safety and efficacy of gasless bilateral axillo-breast approach (BABA) robotic thyroidectomy. Surg Endosc 34, 4846–4856 (2020). https://doi.org/10.1007/s00464-019-07262-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07262-3