
Abstract
Background
MIS utilization for inguinal hernia repair is low compared to in other procedures. The impact of low adoption in surgeons is unclear, but may affect regional access to minimally invasive surgery (MIS). We explored the impact of surgeon MIS utilization in inguinal hernia repair across a statewide population.
Methods
We analyzed 6723 patients undergoing elective inguinal hernia repair from 2012 to 2016 in the Michigan Surgical Quality Collaborative. The primary outcome was surgeon MIS utilization. The geographic distribution of high MIS-utilizing surgeons was compared across Hospital Referral Regions using Pearson’s Chi-squared test. Hierarchical logistic regression was used to identify patient and hospital factors associated with MIS utilization.
Results
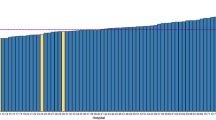
Surgeon MIS utilization varied, with 58% of 540 surgeons performing no MIS repair. For the remaining surgeons, MIS utilization was bimodally distributed. High-utilization surgeons were unevenly distributed across region, with corresponding differences in regional MIS rate ranging from 10 to 48% (p < 0.001). MIS was used in 41% of bilateral and 38% of recurrent hernia. MIS repair was more likely with higher hospital volume and less likely for patients aged 65+ (OR 0.68, p = 0.003), black patients (OR 0.75, p = 0.045), patients with COPD (OR 0.57, p < 0.001), and patients in ASA class > 3 (OR 0.79 p < 0.001).
Conclusions
MIS utilization varies between surgeons, likely driving differences in regional MIS rates and leading to guideline-discordant care for patients with bilateral or recurrent hernia. Interventions to reduce this practice gap could include training programs in MIS repair, or regionalization of care to improve MIS access.


Similar content being viewed by others


References
Smink DS, Paquette IM, Finlayson SR (2009) Utilization of laparoscopic and open inguinal hernia repair: a population-based analysis. J Laparoendosc Adv Surg Tech A 19(6):745–748
Zendejas B, Ramirez T, Jones T et al (2012) Trends in the utilization of inguinal hernia repair techniques: a population-based study. Am J Surg 203(3):313–317
Trevisonno M, Kaneva P, Watanabe Y et al (2015) Current practices of laparoscopic inguinal hernia repair: a population-based analysis. Hernia 19(5):725–733
Ielpo B, Duran H, Diaz E et al (2017) A prospective randomized study comparing laparoscopic transabdominal preperitoneal (TAPP) versus Lichtenstein repair for bilateral inguinal hernias. Am J Surg 216:78–83
Bignell M, Partridge G, Mahon D, Rhodes M (2012) Prospective randomized trial of laparoscopic (transabdominal preperitoneal-TAPP) versus open (mesh) repair for bilateral and recurrent inguinal hernia: incidence of chronic groin pain and impact on quality of life: results of 10 year follow-up. Hernia 16(6):635–640
Bowling K, El-Badawy S, Massri E et al (2017) Laparoscopic and open inguinal hernia repair: patient reported outcomes in the elderly from a single centre—a prospective cohort study. Ann Med Surg 22:12–15
Eker HH, Langeveld HR, Klitsie PJ et al (2012) Randomized clinical trial of total extraperitoneal inguinal hernioplasty vs lichtenstein repair: a long-term follow-up study. Arch Surg 147(3):256–260
McCormack K, Scott NW, Go PM, Ross S, Grant AM (2003) Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Database Syst Rev 2003(1):Cd001785
Abbas AE, Abd Ellatif ME, Noaman N et al (2012) Patient-perspective quality of life after laparoscopic and open hernia repair: a controlled randomized trial. Surg Endosc 26(9):2465–2470
Wang WJ, Chen JZ, Fang Q, Li JF, Jin PF, Li ZT (2013) Comparison of the effects of laparoscopic hernia repair and Lichtenstein tension-free hernia repair. J Laparoendosc Adv Surg Tech A 23(4):301–305
Westin L, Wollert S, Ljungdahl M, Sandblom G, Gunnarsson U, Dahlstrand U (2016) Less pain 1 year after total extra-peritoneal repair compared with lichtenstein using local anesthesia: data from a randomized controlled clinical trial. Ann Surg 263(2):240–243
Simons MP, Aufenacker T, Bay-Nielsen M et al (2009) European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 13(4):343–403
Bittner R, Arregui ME, Bisgaard T et al (2011) Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal Hernia [International Endohernia Society (IEHS)]. Surg Endosc 25(9):2773
Choudhary RK, Hassn AMF (2003) NICE guidance on laparoscopic surgery for inguinal hernias: guidelines are less clinical excellence than hindrance. Br Med J 326(7399):1144–1144
Davis CH, Shirkey BA, Moore LW et al (2018) Trends in laparoscopic colorectal surgery over time from 2005 to 2014 using the NSQIP database. J Surg Res 223:16–21
Tsui C, Klein R, Garabrant M (2013) Minimally invasive surgery: national trends in adoption and future directions for hospital strategy. Surg Endosc 27(7):2253–2257
Hendren S, Fritze D, Banerjee M et al (2013) Antibiotic choice is independently associated with risk of surgical site infection after colectomy: a population-based cohort study. Ann Surg 257(3):469–475
Waits SA, Fritze D, Banerjee M et al (2014) Developing an argument for bundled interventions to reduce surgical site infection in colorectal surgery. Surgery 155(4):602–606
The Center for the Evaluative Clinical Sciences DMS (1996) The Dartmouth atlas of health care. American Hospital Publishing, Chicago
2010 Census Summary File—Michigan (2010) http://www.census.gov/2010census/data/. Accessed 12 Feb 2018
Hernández-Irizarry R, Zendejas B, Ramirez T et al (2012) Trends in emergent inguinal hernia surgery in Olmsted County, MN: a population-based study. Hernia 16(4):397–403
Beadles CA, Meagher AD, Charles AG (2015) Trends in emergent hernia repair in the united states. JAMA Surg 150(3):194–200
Mehta A, Hutfless S, Blair AB et al (2017) Emergency department utilization and predictors of mortality for inpatient inguinal hernia repairs. J Surg Res 212:270–277
Hope WW, Bools L, Menon A, Scott CM 3rd, Adams A, Hooks WB (2013) Comparing laparoscopic and open inguinal hernia repair in octogenarians. Hernia 17(6):719–722
Vigneswaran Y, Gitelis M, Lapin B et al (2015) Elderly and octogenarian cohort: comparable outcomes with nonelderly cohort after open or laparoscopic inguinal hernia repairs. Surgery 158(4):1137–1144
Dallas KB, Froylich D, Choi JJ et al (2013) Laparoscopic versus open inguinal hernia repair in octogenarians: a follow-up study. Geriatr Gerontol Int 13(2):329–333
McCormack K, Wake BL, Fraser C, Vale L, Perez J, Grant A (2005) Transabdominal pre-peritoneal (TAPP) versus totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair: a systematic review. Hernia 9(2):109–114
Physician Fee Schedule Search (2018) https://www.cms.gov/apps/physician-fee-schedule/overview.aspx. Accessed 14 April 2018
Neumayer L, Giobbie-Hurder A, Jonasson O et al (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. New Engl J Med 350(18):1819–1827
Zerey M, Kercher KW, Sing RF et al (2007) Does a one-day course influence surgeon adoption of laparoscopic ventral herniorrhaphy? J Surg Res 138(2):205–208
Greenberg JA, Jolles S, Sullivan S et al (2017) A structured, extended training program to facilitate adoption of new techniques for practicing surgeons. Surg Endosc 32:217–224
Funding
Dr. Vu is funded by the National Institutes of Health T32 Obesity Surgery Scientist Training Program: 1 T32 DK 108740-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Dr. Telem receives consulting fees for Medtronic. Dr. Vu, Ms. Gunaseelan, Dr. Krapohl, Dr. Englesbe, Dr. Campbell, and Dr. Dimick have no conflict of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Vu, J.V., Gunaseelan, V., Krapohl, G.L. et al. Surgeon utilization of minimally invasive techniques for inguinal hernia repair: a population-based study. Surg Endosc 33, 486–493 (2019). https://doi.org/10.1007/s00464-018-6322-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-018-6322-x