
Abstract
Background and study aims
Classic endoscopic resection techniques (EMR and ESD) are limited to mucosal lesions. In the case of deeper growth into the gut wall and anatomic sites prone to perforation, the novel full-thickness resection device (FTRD®) opens a new dimension of possibilities for endoscopic resection.
Patients and methods
Sixty patients underwent endoscopic full-thickness resection (eFTR) at our institution. Safety, learning curve, R0 resection rate, and clinical outcome were studied.
Results
In 97% (58/60) of the interventions, the FTRD®-mounted endoscope reached the previously marked lesion and eFTR was performed (technical success). Full-thickness resection was achieved in 88% of the cases, with an R0 resection on histological examination in 79%. The clinical success rate based on follow-up histology was even higher (88%). Adverse events occurred in 7%. Appendicitis of the residual cecal appendix after eFTR of an adenoma arising in the appendix led to the only post-eFTR surgery (1/58, 2%). Minor bleeding at the eFTR site (2/58, 3%) and an eFTR performed accidently without proper prior deployment of the OTSC® (1/58, 2%) were successfully treated endoscopically. There was no secondary perforation or eFTR-associated mortality.
Conclusions
After specific training, eFTR is a feasible, safe, and promising all-in-one endoscopic resection technique. Our data show that eFTR allows complete resection of lesions affecting layers of the gut wall beneath the mucosa with a low risk of adverse events. However, our preliminary results need to be confirmed in larger, controlled studies.





Similar content being viewed by others

Abbreviations
- EMR:
-
Endoscopic mucosal resection
- ESD:
-
Endoscopic submucosal dissection
- STER:
-
Submucosal tunneling endoscopic resection
- LAEFR:
-
Laparoscopy-assisted endoscopic full-thickness resection
- NOTES:
-
Natural orifice transluminal endoscopic surgery
- GI:
-
Gastrointestinal
- OTSC® :
-
Over-the-scope clip
- FTRD® :
-
Full-thickness resection device
- eFTR:
-
Endoscopic full-thickness resection
References
Maguire LH, Shellito PC (2014) Endoscopic piecemeal resection of large colorectal polyps with long-term followup. Surg Endosc 28:2641–2648
Ye LP, Zhang Y, Mao XL, Zhu LH, Zhou X, Chen JY (2014) Submucosal tunneling endoscopic resection for small upper gastrointestinal subepithelial tumors originating from the muscularis propria layer. Surg Endosc 28:524–530
Lu J, Jiao T, Li Y et al (2015) Heading toward the right direction–solution package for endoscopic submucosal tunneling resection in the stomach. PLoS ONE 10:e0119870
Eleftheriadis N, Inoue H, Ikeda H, Onimaru M, Maselli R, Santi G (2016) Submucosal tunnel endoscopy: peroral endoscopic myotomy and peroral endoscopic tumor resection. World J Gastrointest Endosc 8:86–103
Kuroki Y, Hoteya S, Mitani T et al (2010) Endoscopic submucosal dissection for residual/locally recurrent lesions after endoscopic therapy for colorectal tumors. J Gastroenterol Hepatol 25:1747–1753
Sakamoto T, Saito Y, Matsuda T, Fukunaga S, Nakajima T, Fujii T (2011) Treatment strategy for recurrent or residual colorectal tumors after endoscopic resection. Surg Endosc 25:255–260
Moss A, Williams SJ, Hourigan LF et al (2015) Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut 64:57–65
Abe N, Takeuchi H, Yanagida O et al (2009) Endoscopic full-thickness resection with laparoscopic assistance as hybrid NOTES for gastric submucosal tumor. Surg Endosc 23:1908–1913
Cho WY, Kim YJ, Cho JY et al (2011) Hybrid natural orifice transluminal endoscopic surgery: endoscopic full-thickness resection of early gastric cancer and laparoscopic regional lymph node dissection–14 human cases. Endoscopy 43:134–139
Kirschniak A, Kratt T, Stuker D, Braun A, Schurr MO, Konigsrainer A (2007) A new endoscopic over-the-scope clip system for treatment of lesions and bleeding in the GI tract: first clinical experiences. Gastrointest endosc 66(1):162–167
Honegger C, Valli P, Wiegand N, Bauerfeind P, Gubler C (2016) Establishment of over-the-scope-clips (OTSC®) in daily endoscopic routine. United Eur Gastroenterol J 5(2):247–254
Weiland T, Fehlker M, Gottwald T, Schurr MO (2013) Performance of the OTSC system in the endoscopic closure of iatrogenic gastrointestinal perforations: a systematic review. Surg Endosc 27:2258–2274
Voermans RP, Le Moine O, von Renteln D et al (2012) Efficacy of endoscopic closure of acute perforations of the gastrointestinal tract. Clin Gastroenterol Hepatol 10:603–608
von Renteln D, Schmidt A, Vassiliou MC, Rudolph HU, Gieselmann M, Caca K (2009) Endoscopic closure of large colonic perforations using an over-the-scope clip: a randomized controlled porcine study. Endoscopy 41:481–486
Sarker S, Gutierrez JP, Council L, Brazelton JD, Kyanam Kabir Baig KR, Monkemuller K (2014) Over-the-scope clip-assisted method for resection of full-thickness submucosal lesions of the gastrointestinal tract. Endoscopy 46(9):758–761
von Renteln D, Schmidt A, Vassiliou MC, Rudolph HU, Caca K (2010) Endoscopic full-thickness resection and defect closure in the colon. Gastrointest Endosc 71:1267–1273
Valli PV, Kaufmann M, Vrugt B, Bauerfeind P (2014) Endoscopic resection of a diverticulum-arisen colonic adenoma using a full-thickness resection device. Gastroenterology 147:969–971
Schmidt A, Meier B, Caca K (2015) Endoscopic full-thickness resection: current status. WJG 21:9273–9285
Schmidt A, Bauerfeind P, Gubler C, Damm M, Bauder M, Caca K (2015) Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience. Endoscopy 47:719–725
Schurr MO, Baur F, Ho CN, Anhoeck G, Kratt T, Gottwald T (2011) Endoluminal full-thickness resection of GI lesions: a new device and technique. MITAT 20:189–192
Hassan C, Quintero E, Dumonceau JM et al (2013) Post-polypectomy colonoscopy surveillance: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy 45:842–851
Fahndrich M, Sandmann M (2015) Endoscopic full-thickness resection for gastrointestinal lesions using the over-the-scope clip system: a case series. Endoscopy 47:76–79
Monkemuller K, Peter S, Toshniwal J et al (2014) Multipurpose use of the ‘bear claw’ (over-the-scope-clip system) to treat endoluminal gastrointestinal disorders. Dig Endosc 26:350–357
Xu J, Yang L, Guo Y, Zhao D, Wang L, Bai L (2010) Perforation of sigmoid diverticulum following endoscopic polypectomy of an adenoma. BMJ Case Rep. doi:10.1136/bcr.07.2009.2077
Barr YR, Brazowski E, Leider-Trejo L (2006) Villous adenoma in a perforated colonic diverticulum. Int J Colorectal Dis 21:282–284
Adrales GL, Harold KL, Matthews BD, Sing RF, Kercher KW, Heniford BT (2002) Laparoscopic “radical appendectomy” is an effective alternative to endoscopic removal of cecal polyps. J Laparoendosc Adv Surg Tech A 12:449–452
Denoel C, Legrand MJ, Heymans O, Kunsch JM (2001) Isolated adenomatous polyposis of the appendix: report of a case. Dis Colon Rectum 44:1709–1710
Acknowledgements
We sincerely thank PD Dr. Christoph Gubler for his assistance in the performance of some interventions.
Author contributions
PVV: Editing of results and manuscript, performance of endoscopies. JM: Critical reading and editing of the manuscript. PB: Revision of the manuscript, performance of endoscopies.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
P. V. Vall, J. Mertens, and P. Bauerfeind have no conflicts of interest or financial ties to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
464_2017_5676_MOESM1_ESM.tif
Supplementary material 1 (TIFF 1035 kb). Supplemental Figure 6A Recurrent adenoma after prior polypectomy; B Full-thickness resection specimen, peritoneal face; C Full-thickness resection specimen, adenoma face with all marks included within the resection limits.
464_2017_5676_MOESM2_ESM.tiff
Supplementary material 2 (TIFF 1321 kb). Supplemental Figure 7A Full-thickness resection device (FTRD®), including a hyperthermic snare, running along a standard endoscope; B OTSC® mounted onto a transparent cap containing the resection snare, then fitted on the tip of the endoscope.
464_2017_5676_MOESM3_ESM.tif
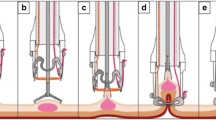
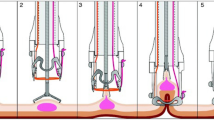
Supplementary material 3 (TIFF 534 kb). Supplemental Figure 8 (kindly provided by Ovesco® Endoscopy AG, Tübingen), step 1: After mounting the FTRD®, the endoscope is advanced to the previously marked lesion; step 2: The target lesion is grabbed with a grasping forceps; step 3: The target lesion is carefully pulled into the plastic cap of the FTRD®, step 4: The OTSC® is deployed; step 5: The eFTR is performed using the hyperthermic snare within the plastic cap.
Rights and permissions
About this article

Cite this article
Valli, P.V., Mertens, J. & Bauerfeind, P. Safe and successful resection of difficult GI lesions using a novel single-step full-thickness resection device (FTRD®). Surg Endosc 32, 289–299 (2018). https://doi.org/10.1007/s00464-017-5676-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5676-9