
Abstract
Background
Previous reports comparing endoscopic therapy (ET) and surgical therapy (ST) have predominantly assessed patients with high-grade dysplasia. The study aim was to compare ET to ST in physiologically fit patients with cT1a adenocarcinoma (EAC).
Methods
Review of two prospective databases yielded 100 patients presenting with clinical cT1a EAC between 2000 and 2013. Only physiologically fit patients who were candidates for either treatment were analyzed.
Results
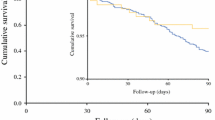
Presenting patient characteristics were similar between ET (n = 36) and ST groups (n = 49). Surgical patients were less likely to be staged with EMR (43 vs 100 %) and were associated with mass lesions >1 cm at EGD (p = 0.01), multifocal EAC (p = 0.03), and positive margins for EAC on EMR (p < 0.05). On multivariate analysis, only multifocal HGD was an independent factor for surgery. Following esophagectomy, R0 resection rates for Barrett’s esophagus and cancer were 100 %. Incidence of surgery decreased over the study period from 85 to 25 %. All ET patients had EMR, and 28 patients underwent additional ablative therapies for Barrett’s esophagus. Following ET, eradication rates of EAC, dysplasia, and BE were 92, 81, and 53 %, respectively. Morbidity rates were comparable between groups (ST 51 % vs ET 39 %, p = 0.31). In-hospital mortality rate was zero in each group. Recurrence rates in ST and ET group were 2 and 11 % (p = 0.08). In the ET group, two patients with endoluminal cancer recurrence after complete eradication underwent esophagectomy. Age-adjusted overall survival was comparable.
Conclusion
In high-volume esophageal centers, ST and ET provide equally safe and effective treatment for cT1a EAC in medically fit patients. While the results of this study provide a historical perspective and clearly demonstrate an evolution toward ET over time, the appropriate treatment modality is best selected in a multidisciplinary fashion with EMR providing the most accurate staging. In endoscopically treated patients, indefinite endoscopic follow-up required, however, standardized long-term follow-up protocols are needed.








Similar content being viewed by others


References
Siegel R, Naishadham D, Jemal A (2012) Cancer statistics, 2012. CA Cancer J Clin 62:10–29
Cen P, Banki F, Cheng L et al (2012) Changes in age, stage distribution, and survival of patients with esophageal adenocarcinoma over three decades in the United States. Ann Surg Oncol 19:1685–1691
Wani S, Drahos J, Cook MB et al (2014) Comparison of endoscopic therapies and surgical resection in patients with early esophageal cancer: a population-based study. Gastrointest Endosc 79:224–232
Pech O, May A, Manner H et al (2014) Long-term efficacy and safety of endoscopic resection for patients with mucosal adenocarcinoma of the esophagus. Gastroenterology 146:652–660
Behrens A, Pech O, Graupe F et al (2011) Barrett’s adenocarcinoma of the esophagus: better outcomes through new methods of diagnosis and treatment. Dtsch Arztebl Int 108:313–319
Holscher AH, Vallbohmer D, Bollschweiler E (2008) Early Barrett’s carcinoma of the esophagus. Ann Thorac Cardiovasc Surg 14:347–354
DeMeester SR (2010) Evaluation and treatment of superficial esophageal cancer. J Gastrointest Surg 14(Suppl 1):S94–S100
Stein HJ, Schweigert M, Dubecz A (2011) Early esophageal cancer: pro surgical resection. Chirurg 82:495–499
Overholt BF, Lightdale CJ, Wang KK et al (2005) Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett’s esophagus: international, partially blinded, randomized phase III trial. Gastrointest Endosc 62:488–498
Shaheen NJ, Sharma P, Overholt BF et al (2009) Radiofrequency ablation in Barrett’s esophagus with dysplasia. N Engl J Med 360:2277–2288
Peters FP, Kara MA, Rosmolen WD et al (2005) Endoscopic treatment of high-grade dysplasia and early stage cancer in Barrett’s esophagus. Gastrointest Endosc 61:506–514
Pech O, Behrens A, May A et al (2008) Long-term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high-grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut 57:1200–1206
Bennett C, Vakil N, Bergman J et al (2012) Consensus statements for management of Barrett’s dysplasia and early-stage esophageal adenocarcinoma, based on a Delphi process. Gastroenterology 143:336–346
Das A, Singh V, Fleischer DE et al (2008) A comparison of endoscopic treatment and surgery in early esophageal cancer: an analysis of surveillance epidemiology and end results data. Am J Gastroenterol 103:1340–1345
Ngamruengphong S, Wolfsen HC, Wallace MB (2013) Survival of patients with superficial esophageal adenocarcinoma after endoscopic treatment vs surgery. Clin Gastroenterol Hepatol 11:1424–1429
Leers JM, DeMeester SR, Oezcelik A et al (2011) The prevalence of lymph node metastases in patients with T1 esophageal adenocarcinoma a retrospective review of esophagectomy specimens. Ann Surg 253:271–278
Stein HJ, Feith M, Bruecher BL et al (2005) Early esophageal cancer: pattern of lymphatic spread and prognostic factors for long-term survival after surgical resection. Ann Surg 242:566–573
Bollschweiler E, Holscher AH (2011) Early adenocarcinoma of the esophagus—clinical relevance of depth of infiltration into the submucosa. Clin Gastroenterol Hepatol 9:277–278
Sepesi B, Watson TJ, Zhou D et al (2010) Are endoscopic therapies appropriate for superficial submucosal esophageal adenocarcinoma? An analysis of esophagectomy specimens. J Am Coll Surg 210:418–427
Ell C, May A, Pech O et al (2007) Curative endoscopic resection of early esophageal adenocarcinomas (Barrett’s cancer). Gastrointest Endosc 65:3–10
Schembre DB, Huang JL, Lin OS et al (2008) Treatment of Barrett’s esophagus with early neoplasia: a comparison of endoscopic therapy and esophagectomy. Gastrointest Endosc 67:595–601
Pech O, May A, Manner H et al (2014) Long-term efficacy and safety of endoscopic resection for patients with mucosal adenocarcinoma of the esophagus. Gastroenterology 146:652–660
Prasad GA, Wu TT, Wigle DA et al (2009) Endoscopic and surgical treatment of mucosal (T1a) esophageal adenocarcinoma in Barrett’s esophagus. Gastroenterology 137:815–823
Pech O, Bollschweiler E, Manner H et al (2011) Comparison between endoscopic and surgical resection of mucosal esophageal adenocarcinoma in Barrett’s esophagus at two high-volume centers. Ann Surg 254:67–72
Schembre DB (2009) Endotherapy for Barrett’s esophagus with high-grade dysplasia and intramucosal carcinoma. J Gastrointest Surg 13:1172–1178
Levine DS, Haggitt RC, Blount PL et al (1993) An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s esophagus. Gastroenterology 105:40–50
Markar SR, Schmidt H, Kunz S et al (2014) Evolution of standardized clinical pathways: refining multidisciplinary care and process to improve outcomes of the surgical treatment of esophageal cancer. J Gastrointest Surg 18:1238–1246
Williams VA, Watson TJ, Herbella FA et al (2007) Esophagectomy for high grade dysplasia is safe, curative, and results in good alimentary outcome. J Gastrointest Surg 11:1589–1597
Mino-Kenudson M, Hull MJ, Brown I et al (2007) EMR for Barrett’s esophagus-related superficial neoplasms offers better diagnostic reproducibility than mucosal biopsy. Gastrointest Endosc 66:660–666
Pech O, Manner H, Ell C (2011) Endoscopic resection. Gastrointest Endosc Clin N Am 21:81–94
Pech O, Gunter E, Ell C (2009) Endosonography of high-grade intra-epithelial neoplasia/early cancer. Best Pract Res Clin Gastroenterol 23:639–647
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Henner M. Schmidt, Kamran Mohiuddin, Artur M. Bodnar, Mustapha El Lakis, Stephen Kaplan, Shayan Irani, Ian Gan, Andrew Ross, and Donald E. Low have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Schmidt, H.M., Mohiuddin, K., Bodnar, A.M. et al. Multidisciplinary treatment of T1a adenocarcinoma in Barrett’s esophagus: contemporary comparison of endoscopic and surgical treatment in physiologically fit patients. Surg Endosc 30, 3391–3401 (2016). https://doi.org/10.1007/s00464-015-4621-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4621-z