
Abstract
Background
Laparoscopic repair of paraesophageal hernia (PEH) with fundoplication is currently the preferred elective strategy, but emergent cases are often done open without an anti-reflux (AR) procedure. This study examined PEH repair in elective and urgent/emergent settings and investigated patient characteristic influence on the use of adjunctive techniques, such as AR procedures or gastrostomy tube (GT) placement.
Methods
Utilizing the University HealthSystem Consortium Clinical Database Resource Manager, selected discharge data were retrieved using International Classification of Disease 9 diagnosis codes for PEH and procedure specific codes. Chi-squared and paired t tests were applied (α = 0.05).
Results
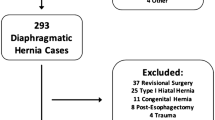
Discharge data from October 2010 through June 2014 indicated 7950 patients (≥18 years) underwent PEH surgery, 84.7 % were performed laparoscopically and 15.3 % open. 24.6 % of cases were classified urgent/emergent upon admission, and almost 70 % of these were completed laparoscopically. Open paraesophageal hernia repairs (OHR) represented a higher proportion of urgent/emergent cases but were only 30 % of this total. Laparoscopic paraesophageal hernia repair (LHR) patients were more likely to receive an AR procedure in all situations (54.9 % LHR vs. 26.3 % OHR). Almost 90 % of elective PEH repairs in this cohort were laparoscopic. Elective cases were more commonly associated with AR procedures than emergent cases which frequently incorporated GT placement.
Conclusion
We demonstrate that laparoscopic PEH repair has become accepted in emergent cases. Open PEH repair is often reserved for emergent surgeries and less commonly includes an AR procedure. Laparoscopy with an AR procedure is clearly the standard of care in elective surgery. The decision to perform an open or laparoscopic surgery, with or without adjunctive techniques, may be based more on the physician’s comfort with laparoscopic surgery and surgical practices than the patient’s condition. Long-term follow-up studies are needed to determine the functional outcomes of these strategies.
Similar content being viewed by others


References
Allison PR (1951) Reflux esophagitis, sliding hiatal hernia, and the anatomy of repair. Surg Gynecol Obstet 92:419–431
Allison PR (1973) Hiatus hernia: (a 20-year retrospective survey). Ann Surg 178:273–276
DeMeester SR (2013) Laparoscopic paraesophageal hernia repair: critical steps and adjunct techniques to minimize recurrence. Surg Laparosc Endosc Percutan Tech 23:429–435. doi:10.1097/SLE.0b013e3182a12716
Nguyen NT, Christie C, Masoomi H, Matin T, Laugenour K, Hohmann S (2011) Utilization and outcomes of laparoscopic versus open paraesophageal hernia repair. Am Surg 77:1353–1357
Parker DM, Rambhajan A, Johanson K, Ibele A, Gabrielsen JD, Petrick AT (2013) Urgent laparoscopic repair of acutely symptomatic PEH is safe and effective. Surg Endosc 27:4081–4086. doi:10.1007/s00464-013-3064-7
UHC Clinical Data Base/Resource Manager™. Chicago, IL: UHC; 2012. https://www.uhc.edu. Accessed 2010–2015 for data from October 2010 through October 2014
Holm S (1979) A simple sequentially rejective multiple test procedure. Scand J Stat 6:65–70
Gaetano J (2013) Holm–Bonferroni correction: an Excel calculator-ver. 1.2. 2015. http://www.researchgate.net/profile/Justin_Gaetano2/. Accessed July 2014.
Draaisma WA, Gooszen HG, Tournoij E, Broeders IA (2005) Controversies in paraesophageal hernia repair: a review of literature. Surg Endosc 19:1300–1308. doi:10.1007/s00464-004-2275-3
Jones R, Simorov A, Lomelin D, Tadaki C, Oleynikov D (2014) Long-term outcomes of radiologic recurrence after paraesophageal hernia repair with mesh. Surg Endosc. doi:10.1007/s00464-014-3690-8
Granderath FA, Carlson MA, Champion JK, Szold A, Basso N, Pointner R, Frantzides CT (2006) Prosthetic closure of the esophageal hiatus in large hiatal hernia repair and laparoscopic antireflux surgery. Surg Endosc 20:367–379. doi:10.1007/s00464-005-0467-0
Auyang ED, Oelschlager BK (2013) Laparoscopic paraesophageal hernia repair. In: Swanstrom LL, Soper NJ (eds) Mastery of Endoscopic and Laparoscopic Surgery, 4th edn. Lippincott Williams and Wilkins, Philadelphia, pp 222–230
Simorov A, Ranade A, Jones R, Tadaki C, Shostrom V, Boilesen E, Oleynikov D (2014) Long-term patient outcomes after laparoscopic anti-reflux procedures. J Gastrointest Surg 18:157–162; discussion 162–163, doi:10.1007/s11605-013-2401-4
Furnee EJ, Draaisma WA, Gooszen HG, Hazebroek EJ, Smout AJ, Broeders IA (2011) Tailored or routine addition of an antireflux fundoplication in laparoscopic large hiatal hernia repair: a comparative cohort study. World J Surg 35:78–84. doi:10.1007/s00268-010-0814-8
Funding Source
The authors acknowledge support from The Center for Advanced Surgical Technology at the University of Nebraska Medical Center and the Foundation for Surgical Fellows.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Michael Klinginsmith, Jennifer Jolley, Daniel Lomelin, Crystal Krause, Jace Heiden, Dmitry Oleynikov have no conflict of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Klinginsmith, M., Jolley, J., Lomelin, D. et al. Paraesophageal hernia repair in the emergency setting: is laparoscopy with the addition of a fundoplication the new gold standard?. Surg Endosc 30, 1790–1795 (2016). https://doi.org/10.1007/s00464-015-4447-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4447-8