
Abstract
Background
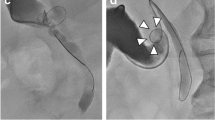
When common bile duct (CBD) stones are detected during laparoscopic cholecystectomy, the insertion of baskets via the cystic duct (CD) can be difficult and may occasionally cause complications. We introduced a new technique ‘basket in catheter’ (BIC) for transcystic CBD exploration.
Methods
Although cannulating the CD using a cholangiography catheter is successful in most cases, it may occasionally be difficult. Cystic duct anatomy may prevent the usually stiffer sharper tip of the basket, from entering the CBD, resulting in failure, perforation or a false passage. In the majority of our cases, the cholangiography catheter (CC) is not withdrawn from the duct should the intraoperative cholangiography show CBD stones. The tip of a basket is inserted into the CC and advanced to a predetermined distance, allowing the tip of the basket to exit the end of the CC into the CBD. The basket is then opened, advanced to feel the lower end and manipulated to trap the stone. The common hepatic duct is compressed gently to prevent stones from slipping upwards. The catheter and basket are pulled back together to extract the stone.
Results
We have used this technique in 274 cases since 2010. The rate of transcystic versus choledochotomy stone extraction has increased, saving unnecessary choledochotomies. The percentage of transcystic exploration increased from 55 % for the period 2005–2009 to 70 % for the period 2010–2014. There were no conversions to open surgery and no retained stones. The morbidity rate was 4.0 % with no mortality.
Conclusions
We demonstrate a technique to facilitate the insertion of extraction baskets into the common bile duct using the cholangiography catheter as a guide. The ‘basket-in-catheter’ (BIC) technique for transcystic CBD exploration is easier and safer than inserting the basket alone.






Similar content being viewed by others


References
Pitt HA (1993) Role of open choledochotomy in the treatment of choledocholithiasis. Am J Surg 165:483–486
Hermann RE (1989) The spectrum of biliary stone disease. Am J Surg 158:171–173
Way LW, Admirand WH, Dunphy JE (1972) Management of choledocholithiasis. Ann Surg 176:347–359
Clayton ES, Connor S, Alexakis N, Leandros E (2006) Meta-analysis of endoscopy and surgery versus surgery alone for common bile duct stones with the gallbladder in situ. Br J Surg 93:1185–1191. doi:10.1002/bjs.5568
Dasari BV, Tan CJ, Gurusamy KS, Martin DJ, Kirk G, McKie L, Diamond T, Taylor MA (2013) Surgical versus endoscopic treatment of bile duct stones. Cochrane Database Syst Rev 12:CD003327. doi:10.1002/14651858.CD003327.pub4
Poulose BK, Arbogast PG, Holzman MD (2006) National analysis of in-hospital resource utilization in choledocholithiasis management using propensity scores. Surg Endosc 20:186–190. doi:10.1007/s00464-005-0235-1
Hanif F, Ahmed Z, Samie MA, Nassar AH (2010) Laparoscopic transcystic bile duct exploration: the treatment of first choice for common bile duct stones. Surg Endosc 24:1552–1556. doi:10.1007/s00464-009-0809-4
Prat F, Amouyal G, Amouyal P, Pelletier G, Fritsch J, Choury AD, Buffet C, Etienne JP (1996) Prospective controlled study of endoscopic ultrasonography and endoscopic retrograde cholangiography in patients with suspected common-bileduct lithiasis. Lancet 347:75–79
Trondsen E, Edwin B, Reiertsen O, Faerden AE, Fagertun H, Rosseland AR (1998) Prediction of common bile duct stones prior to cholecystectomy: a prospective validation of a discriminant analysis function. Arch Surg 133:162–166
Liu TH, Consorti ET, Kawashima A, Tamm EP, Kwong KL, Gill BS, Sellin JH, Peden EK, Mercer DW (2001) Patient evaluation and management with selective use of magnetic resonance cholangiography and endoscopic retrograde cholangiopancreatography before laparoscopic cholecystectomy. Ann Surg 234:33–40
Joyce WP, Keane R, Burke GJ, Daly M, Drumm J, Egan TJ, Delaney PV (1991) Identification of bile duct stones in patients undergoing laparoscopic cholecystectomy. Br J Surg 78:1174–1176
Cetta F (1993) Do surgical and endoscopic sphincterotomy prevent or facilitate recurrent common duct stone formation? Arch Surg 128:329–336
Hamouda AH, Goh W, Mahmud S, Khan M, Nassar AH (2007) Intraoperative cholangiography facilitates simple transcystic clearance of ductal stones in units without expertise for laparoscopic bile duct surgery. Surg Endosc 21:955–959. doi:10.1007/s00464-006-9127-2
Nassar AH, El Shallaly G, Hamouda AH (2009) Optimising laparoscopic cholangiography time using a simple cannulation technique. Surg Endosc 23:513–517. doi:10.1007/s00464-008-9853-8
Gough V, Stephens N, Ahmed Z, Nassar AH (2012) Intrahepatic choledochoscopy during trans-cystic common bile duct exploration; technique, feasibility and value. Surg Endosc 26:3190–3194. doi:10.1007/s00464-012-2315-3
Collins C, Maguire D, Ireland A, Fitzgerald E, O’Sullivan GC (2004) A prospective study of common bile duct calculi in patients undergoing laparoscopic cholecystectomy: natural history of choledocholithiasis revisited. Ann Surg 239:28–33. doi:10.1097/01.sla.0000103069.00170.9c
Gologan E, Balan G, Stanciu C (2006) Conventional ultrasound in the diagnosis of bile duct calculi. Rev Med Chir Soc Med Nat Iasi 110:824–829
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Haitham Qandeel, Samer Zino, Zulfiqar Hanif, M. Kazem Nassar and Ahmad H. M. Nassar have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Qandeel, H., Zino, S., Hanif, Z. et al. Basket-in-catheter access for transcystic laparoscopic bile duct exploration: technique and results. Surg Endosc 30, 1958–1964 (2016). https://doi.org/10.1007/s00464-015-4421-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4421-5