
Abstract
Background
Endoscopic mucosal resection (EMR) or radical surgical resection are the standard treatment options for patients with early Barrett´s adenocarcinoma (EBAC). Endoscopic submucosal dissection (ESD) is a new endoscopic technique, which allows—in contrast to EMR—endoscopic en-bloc resection of neoplastic lesions greater than 2 cm with complete histological evaluation of the resected specimen. In contrast to Western countries, Barrett´s esophagus is less common in Asia indicating the low volume of published data of ESD in EBAC in Japanese series. Therefore, the aim of the present study is to describe the results of ESD in patients with EBAC performed in a German tertiary referral center.
Methods
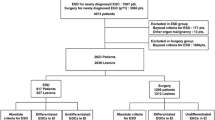
Between November 2009 and April 2014 ESDs were performed in 22 patients with histologically proven EBAC. Data were given for the en-bloc, the R0, the R0 en-bloc, and the curative resection rate as well as for the complication and the local recurrence rate.
Results
ESD was technically possible in all of the 22 patients. 20 of the resected EBAC were mucosal carcinomas, whereas in two patients the tumor showed submucosal invasion. The en-bloc, R0, R0 en-bloc, and curative resection rates were 95.5, 81.8, 81.8 %, and77.3 %, resp. Complication rate was 27.3 % (perforation n = 1, bleeding n = 2, stenosis n = 3). In case of curative tumor resection, only one local tumor recurrence (5.9 %) occurred after a medium follow-up of 1.6 years.
Conclusions
Despite the small number of patients and a relatively short follow-up, the present data underline the value of ESD, especially in case of curative resections in the definite and less invasive therapy of EBAC. Attention should be drawn toward subsquamous extension of EBAC requiring a sufficient safety margin as an obligate condition for curative R0 resections. Due to the required learning curve and the management of potential complications, ESD should be restricted to greater endoscopic centers.



Similar content being viewed by others


References
Pohl H, Welch HG (2005) The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst 97:142–146
Gaddam S, Singh M, Balasubramanian G, Thota P, Gupta N, Wani S, Higbee AD, Mathur SC, Horwhat JD, Rastogi A, Young PE, Cash BD, Bansal A, Vargo JJ, Falk GW, Lieberman DA, Sampliner RE, Sharma P (2013) Persistence of nondysplastic Barrett’s esophagus identifies patients at lower risk for esophageal adenocarcinoma: results from a large multicenter cohort. Gastroenterology 145:548–553
Sharma P (2009) Clinical practice. Barrett’s esophagus. N Engl J Med 361:2548–2556
Peitz U, Malfertheiner P (2007) Barrett carcinoma: diagnosis, screening, surveillance, endoscopic treatment, prevention. Z Gastroenterol 45(12):1264–1272
Sharma P, Falk GW, Weston AP, Reker D, Johnston M, Sampliner RE (2006) Dysplasia and cancer in a large multicenter cohort of patients with Barrett’s esophagus. Clin Gastroenterol Hepatol 4(5):566–572
Kubo A, Corley DA, Jensen CD, Kaur R (2010) Dietary factors and the risks of oesophageal adenocarcinoma and Barrett’s oesophagus. Nutr Res Rev 23(2):230–246
Pech O, Bollschweiler E, Manner H, Leers J, Ell C, Hölscher H (2011) Comparison between endoscopic and surgical resection of mucosal esophageal adenocarcinoma in Barrett´s esophagus at two high-volume centers. Ann Surg 254:67–72
Probst A, Golder D, Arnholdt H, Messmann H (2009) Endoscopic submucosal dissection of early cancers, flat adenomas, and submucosal tumors in the gastrointestinal tract. Clin Gastroenterol Hepatol 7(2):149–155
Wang KK, Prasad G, Tian J (2010) Endoscopic mucosal resection and endoscopic submucosal dissection in esophageal and gastric cancers. Curr Opin Gastroenterol 26(5):453–458
Muto M, Manabe T, Ohtsu A, Yoshida S (2005) Local recurrence of squamous-cell carcinoma of the esophagus. Gastrointest Endosc 61:219–225
Ortiz-Fernández-Sordo J, Parra-Blanco A, García-Varona A, Rodríguez-Peláez M, Madrigal-Hoyos E, Waxman I, Rodrigo L (2011) Endoscopic resection techniques and ablative therapies for Barrett’s neoplasia. World J Gastrointest Endosc 3(9):71–182
Ono S, Fujishiro M, Koike K (2012) Endoscopic submucosal dissection for superficial esophageal neoplasms. World J Gastrointest Endosc 4(5):162–166
Miyamoto S, Muto M, Hamamoto Y, Boku N, Ohtsu A, Baba S, Yoshida M, Ohkuwa M, Hosokawa K, Tajiri H, Yoshida S (2002) A new technique for endoscopic mucosal resection with an insulated-tip electrosurgical knife improves the completeness of resection of intramucosal gastric neoplasms. Gastrointest Endosc 55(4):576–581
Yamamoto HKH, Sunada K (2003) Successful en-bloc-resection of large superficial tumors in the stomach and colon using sodium hyaluronate and small caliber-tip-transparent hood. Endoscopy 35:690–694
Höbel S, Baumbach R, Dautel P, Oldhafer KJ, Stang A, Feyerabend B, Yahagi N, Faiss S (2014) Single centre experience of endoscopic submucosal dissection (ESD) in premalignant and malignant gastrointestinal neoplasia. Z Gastroenterol 52:193–199
Toyonaga T, Man-i M, East JE, Nishino E, Ono W, Hirooka T, Ueda C, Iwata Y, Sugiyama T, Dozaiku T, Hirooka T, Fujita T, Inokuchi H, Azuma T (2013) 1,635 Endoscopic submucosal dissection cases in the esophagus, stomach, and colorectum: complication rates and long-term outcomes. Surg Endosc 27(3):1000–1008
Neuhaus H, Terheggen G, Rutz EM, Vieth M, Schumacher B (2012) Endoscopic submucosal dissection plus radiofrequency ablation of neoplastic Barrett’s esophagus. Endoscopy 44:1105–1113
Asano M (2012) Endoscopic submucosal dissection and surgical treatment for gastrointestinal cancer. World J Gastrointest Endosc 4(10):438–447
Hirasawa K, Kokawa A, Oka H, Yahara S, Sasaki T, Nozawa A, Tanaka K (2010) Superficial adenocarcinoma of the esophagogastric junction: long-term results of endoscopic submucosal dissection. Gastrointest Endosc 72(5):960–966
Anders M, Lucks Y, El-Masry MA, Quaas A, Rösch T, Schachschal G, Bähr C, Gauger U, Sauter G, Izbicki JR, Marx AH (2014) Subsquamous extension of intestinal metaplasia is detected in 98% of cases of neoplastic Barrett’s esophagus. Clin Gastroenterol Hepatol 12(3):405–410
Ono S, Fujishiro M, Niimi K, Goto O, Kodashima S, Yamamichi N, Omata M (2009) Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest Endosc 70(5):860–866
Ishii N, Horiki N, Itoh T, Uemura M, Maruyama M, Suzuki S, Uchida S, Izuka Y, Fukuda K, Fujita Y (2010) Endoscopic submucosal dissection with a combination of small-caliber-tip transparent hood and flex knife is a safe and effective treatment for superficial esophageal neoplasias. Surg Endosc 24(2):335–342
Repici A, Hassan C, Carlino A, Pagano N, Zullo A, Rando G, Strangio G, Romeo F, Nicita R, Rosati R, Malesci A (2010) Endoscopic submucosal dissection in patients with early esophageal squamous cell carcinoma: results from a prospective Western series. Gastrointest Endosc 71(4):715–721
Fujishiro M, Yahagi N, Kakushima N, Kodashima S, Muraki Y, Ono S, Yamamichi N, Tateishi A, Shimizu Y, Oka M, Ogura K, Kawabe T, Ichinose M, Omata M (2006) Endoscopic submucosal dissection of esophageal squamous cell neoplasms. Clin Gastroenterol Hepatol 4(6):688–694
Fujishiro M, Kodashima S (2009) Indications, techniques, and outcomes of endoscopic submucosal dissection for esophageal squamous cell carcinoma. Esophagus 6(3):143–148
Disclosure
Dr. P. Dautel, Dr. R. Baumbach, Dr. S. Faiss became speaker honoraria from Olympus Deutschland GmbH (Hamburg, Deutschland). Dr. N. Yahagi became speaker honoraria and honoraria for consultantship from Olympus (Tokyo, Japan). Dr. S. Höbel, Dr. K.-J. Oldhafer, Dr. A. Stang, Dr. B. Feyerabend, Dr. C. Schrader have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Höbel, S., Dautel, P., Baumbach, R. et al. Single center experience of endoscopic submucosal dissection (ESD) in early Barrett´s adenocarcinoma. Surg Endosc 29, 1591–1597 (2015). https://doi.org/10.1007/s00464-014-3847-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3847-5