
Abstract
Background
During laparoscopic cholecystectomy, common bile duct (CBD) injury is a rare but severe complication. To reduce the risk of injury, near-infrared (NIR) fluorescent cholangiography using indocyanine green (ICG) has recently been introduced as a novel method of visualizing the biliary system during surgery. To date, several studies have shown feasibility of this technique; however, liver background fluorescence remains a major problem during fluorescent cholangiography. The aim of the current study was to optimize ICG dose and timing for NIR cholangiography using a quantitative intraoperative camera system during open hepatopancreatobiliary (HPB) surgery. Subsequently, these results were validated during laparoscopic cholecystectomy using a laparoscopic fluorescence imaging system.
Methods
Twenty-seven patients who underwent NIR imaging using the Mini-FLARE image-guided surgery system during open HPB surgery were analyzed to assess optimal dosage and timing of ICG administration. ICG was intravenously injected preoperatively at doses of 5, 10, and 20 mg, and imaged at either 30 min (early) or 24 h (delayed) post-injection. Next, the optimal doses found for early and delayed imaging were applied to two groups of seven patients (n = 14) undergoing laparoscopic NIR fluorescent cholangiography during laparoscopic cholecystectomy.
Results
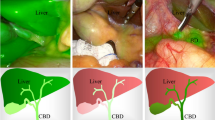
Median liver-to-background contrast was 23.5 (range 22.1–35.0), 16.8 (range 11.3–25.1), 1.3 (range 0.7–7.8), and 2.5 (range 1.3–3.6) for 5 mg/30 min, 10 mg/30 min, 10 mg/24 h, and 20 mg/24 h, respectively. Fluorescence intensity of the liver was significantly lower in the 10 mg delayed-imaging dose group compared with the early imaging 5 and 10 mg dose groups (p = 0.001), which resulted in a significant increase in CBD-to-liver contrast ratio compared with the early administration groups (p < 0.002). These findings were qualitatively confirmed during laparoscopic cholecystectomy.
Conclusion
This study shows that a prolonged interval between ICG administration and surgery permits optimal NIR cholangiography with minimal liver background fluorescence.




Similar content being viewed by others


References
NIH Consensus conference. Gallstones and laparoscopic cholecystectomy. JAMA 269:1018–1024(1993)
Perissat J (1993) Laparoscopic cholecystectomy: the European experience. Am J Surg 165:444–449
Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko ST, Airan MC (1993) Complications of laparoscopic cholecystectomy: a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg 165:9–14
Flum DR, Koepsell T, Heagerty P, Sinanan M, Dellinger EP (2001) Common bile duct injury during laparoscopic cholecystectomy and the use of intraoperative cholangiography: adverse outcome or preventable error? Arch Surg 136:1287–1292
Giger U, Ouaissi M, Schmitz SF, Krahenbuhl S, Krahenbuhl L (2011) Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg 98:391–396
Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T (2003) Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 289:1639–1644
Ford JA, Soop M, Du J, Loveday BP, Rodgers M (2012) Systematic review of intraoperative cholangiography in cholecystectomy. Br J Surg 99:160–167
Ausania F, Holmes LR, Ausania F, Iype S, Ricci P, White SA (2012) Intraoperative cholangiography in the laparoscopic cholecystectomy era: why are we still debating? Surg Endosc 26:1193–1200
Ishizawa T, Bandai Y, Ijichi M, Kaneko J, Hasegawa K, Kokudo N (2010) Fluorescent cholangiography illuminating the biliary tree during laparoscopic cholecystectomy. Br J Surg 97:1369–1377
Aoki T, Murakami M, Yasuda D, Shimizu Y, Kusano T, Matsuda K, Niiya T, Kato H, Murai N, Otsuka K, Kusano M, Kato T (2009) Intraoperative fluorescent imaging using indocyanine green for liver mapping and cholangiography. J Hepatobiliary Pancreat Surg 17:590–594
Schols RM, Bouvy ND, Masclee AA, van Dam RM, Dejong CH, Stassen LP (2013) Fluorescence cholangiography during laparoscopic cholecystectomy: a feasibility study on early biliary tract delineation. Surg Endosc 27:1530–1536
Cherrick GR, Stein SW, Leevy CM, Davidson CS (1960) Indocyanine green: observations on its physical properties, plasma decay, and hepatic extraction. J Clin Invest 39:592–600
Schols RM, Bouvy ND, van Dam RM, Stassen LP (2013) Advanced intraoperative imaging methods for laparoscopic anatomy navigation: an overview. Surg Endosc 27:1851–1859
Gioux S, Choi HS, Frangioni JV (2010) Image-guided surgery using invisible near-infrared light: fundamentals of clinical translation. Mol Imaging 9:237–255
Verbeek FP, van der Vorst JR, Schaafsma BE, Hutteman M, Bonsing BA, van Leeuwen FW, Frangioni JV, van de Velde CJ, Swijnenburg RJ, Vahrmeijer AL (2012) Image-guided hepatopancreatobiliary surgery using near-infrared fluorescent light. J Hepatobiliary Pancreat Sci 19:626–637
Mieog JS, Troyan SL, Hutteman M, Donohue KJ, van der Vorst JR, Stockdale A, Liefers GJ, Choi HS, Gibbs-Strauss SL, Putter H, Gioux S, Kuppen PJ, Ashitate Y, Löwik CW, Smit VT, Oketokoun R, Ngo LH, van de Velde CJ, Frangioni JV, Vahrmeijer AL (2011) Towards optimization of imaging system and lymphatic tracer for near-infrared fluorescent sentinel lymph node mapping in breast cancer. Ann Surg Oncol 18:2483–2491
Tanaka E, Choi HS, Humblet V, Ohnishi S, Laurence RG, Frangioni JV (2008) Real-time intraoperative assessment of the extrahepatic bile ducts in rats and pigs using invisible near-infrared fluorescent light. Surgery 144:39–48
Hutteman M, van der Vorst JR, Mieog JS, Bonsing BA, Hartgrink HH, Kuppen PJ, Lowik CW, Frangioni JV, van de Velde CJ, Vahrmeijer AL (2011) Near-infrared fluorescence imaging in patients undergoing pancreaticoduodenectomy. Eur Surg Res 47:90–97
Mitsuhashi N, Kimura F, Shimizu H, Imamaki M, Yoshidome H, Ohtsuka M, Kato A, Yoshitomi H, Nozawa S, Furukawa K, Takeuchi D, Takayashiki T, Suda K, Igarashi T, Miyazaki M (2008) Usefulness of intraoperative fluorescence imaging to evaluate local anatomy in hepatobiliary surgery. J Hepatobiliary Pancreat Surg 15:508–514
Mizuno S, Isaji S (2010) Indocyanine green (ICG) fluorescence imaging-guided cholangiography for donor hepatectomy in living donor liver transplantation. Am J Transplant 10:2725–2726
Ishizawa T, Tamura S, Masuda K, Aoki T, Hasegawa K, Imamura H, Beck Y, Kokudo N (2009) Intraoperative fluorescent cholangiography using indocyanine green: a biliary road map for safe surgery. J Am Coll Surg 208:e1–e4
Ishizawa T, Bandai Y, Kokudo N (2009) Fluorescent cholangiography using indocyanine green for laparoscopic cholecystectomy: an initial experience. Arch Surg 144:381–382
Kawaguchi Y, Ishizawa T, Masuda K, Sato S, Kaneko J, Aoki T, Beck Y, Sugawara Y, Hasegawa K, Kokudo N (2011) Hepatobiliary surgery guided by a novel fluorescent imaging technique for visualizing hepatic arteries, bile ducts, and liver cancers on color images. J Am Coll Surg 212:e33–e39
Tagaya N, Shimoda M, Kato M, Nakagawa A, Abe A, Iwasaki Y, Oishi H, Shirotani N, Kubota K (2009) Intraoperative exploration of biliary anatomy using fluorescence imaging of indocyanine green in experimental and clinical cholecystectomies. J Hepatobiliary Pancreat Surg 17:595–600
Ishizawa T, Kaneko J, Inoue Y, Takemura N, Seyama Y, Aoki T, Beck Y, Sugawara Y, Hasegawa K, Harada N, Ijichi M, Kusaka K, Shibasaki M, Bandai Y, Kokudo N (2011) Application of fluorescent cholangiography to single-incision laparoscopic cholecystectomy. Surg Endosc 25:2631–2636
Buchs NC, Pugin F, Azagury DE, Jung M, Volonte F, Hagen ME, Morel P (2013) Real-time near-infrared fluorescent cholangiography could shorten operative time during robotic single-site cholecystectomy. Surg Endosc 27:3897–3901
Ashitate Y, Stockdale A, Choi HS, Laurence RG, Frangioni JV (2011) Real-time simultaneous near-infrared fluorescence imaging of bile duct and arterial anatomy. J Surg Res 176(1):7–13
Matsui A, Tanaka E, Choi HS, Winer JH, Kianzad V, Gioux S, Laurence RG, Frangioni JV (2010) Real-time intra-operative near-infrared fluorescence identification of the extrahepatic bile ducts using clinically available contrast agents. Surgery 148:87–95
Sherwinter DA (2012) Identification of anomolous biliary anatomy using near-infrared cholangiography. J Gastrointest Surg 16:1814–1815
Acknowledgments
We thank David Burrington Jr. for editing this manuscript. This work was supported in part by the Dutch Cancer Society Grant UL2010-4732. Research reported in this publication was also supported by the National Institutes of Health grant R01-CA-115296.
Disclosures
Dr. John V. Frangioni declares the following: FLARE™ technology is owned by Beth Israel Deaconess Medical Center, a teaching hospital of Harvard Medical School. It has been licensed to the FLARE™ Foundation, a non-profit organization focused on promoting the dissemination of medical imaging technology for research and clinical use. Dr. Frangioni is the founder and chairman of the FLARE™ Foundation. The Beth Israel Deaconess Medical Center will receive royalties for the sale of FLARE™ Technology. Dr. Frangioni has elected to surrender post-market royalties to which he would otherwise be entitled as inventor, and has elected to donate pre-market proceeds to the FLARE™ Foundation. Floris P. R. Verbeek, Boudewijn E. Schaafsma, Quirijn R.J.G. Tummers, Joost R. van der Vorst, Wendeline J. van der Made, Coen I. Baeten, Bert A. Bonsing, Cornelius J. H. van de Velde, Alexander L. Vahrmeijer and Rutger-Jan Swijnenburg have no conflicts of interest or financial ties to disclose.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Verbeek, F.P.R., Schaafsma, B.E., Tummers, Q.R.J.G. et al. Optimization of near-infrared fluorescence cholangiography for open and laparoscopic surgery. Surg Endosc 28, 1076–1082 (2014). https://doi.org/10.1007/s00464-013-3305-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3305-9