
Abstract
Background
Urologists have not reached a consensus regarding the pre-, intra-, and postoperative management of patients taking antiplatelet agents. This study aimed to evaluate the clinical course of patients receiving antithrombotic monotherapy with acetylsalicylic acid (ASA) 100 mg who underwent transurethral resection of bladder cancer.
Methods
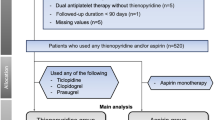
This study was designed to compare the surgical outcomes for 108 transurethral resections of bladder cancer performed for patients taking antiplatelet therapy and for 105 procedures performed for patients who had never taken antiplatelet agents before surgery. Antiaggregant therapy was maintained according to criteria evaluated by a urologist, surgeon, anesthesiologist, and cardiologist. Variables were described using the mean as the location index and using standard deviation as a dispersion index if continuous percentages were used elsewhere. Group comparisons were performed using the t test or the chi-square test for categorical data, and Fisher’s exact test was used where appropriate.
Results
The mean operative time for patients taking ASA was 31 min (range 10–65 min), whereas it was 26 min (range 5–60 min) for control subjects. The difference between pre- and postoperative hemoglobin values was −0.6 g/dl in the group receiving antiplatelet therapy and −0.8 g/dl in the control group (p = 0.0720). Transfusional support was required during four procedures performed for patients taking antiplatelet therapy and during two procedures for the control group (p = 0.242). No adverse cardiac events or anesthesia-related complications occurred. Three patients in the treatment group and two patients in the control group required reintervention to ensure hemostasis during the postoperative period. None of the patients in either group underwent rehospitalization for hematuria after leaving the hospital.
Conclusion
The current results suggest that continued use of anti-aggregant monotherapy does not increase the risk of overall bleeding or reintervention for patients undergoing transurethral resection of bladder neoplasms and that suspending aspirin before such a procedure is therefore unnecessary.
Similar content being viewed by others


References
Möllmann H, Nef HM, Hamm CW, Elsässer A (2009) How to manage patients with need for antiplatelet therapy in the setting of (un)planned surgery. Clin Res Cardiol 98:8–15
Eberli D, Chassot PG, Sulser T et al (2010) Urological surgery and antiplatelet drugs after cardiac and cerebrovascular accidents. J Urol 183:2128–2136
Antithrombotic Trialists’ Collaboration (2002) Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high-risk patients. BMJ 324:71–86
SAS Institute Inc., SAS 9.2 (2000–2004) Help and documentation. SAS Institute Inc., Cary
Carmignani L, Picozzi S, Bozzini G et al (2011) Transrectal ultrasound-guided prostate biopsies in patients taking aspirin for cardiovascular disease: a meta-analysis. Transfus Apher Sci 45:275–280
Enver MK, Hoh I, Chinegwundoh FI (2006) The management of aspirin in transurethral prostatectomy: current practice in the UK. Ann R Coll Surg Engl 88:280–283
Taylor K, Filgate R, Guo DY, Macneil F (2011) A retrospective study to assess the morbidity associated with transurethral prostatectomy in patients on antiplatelet or anticoagulant drugs. BJU Int 108:45–50
Turna B, Stein RJ, Smaldone MC et al (2008) Safety and efficacy of flexible ureterorenoscopy and holmium: YAG lithotripsy for intrarenal stones in anticoagulated cases. J Urol 179:1415–1419
Vasudeva P, Goel A, Sengottayan VK, Sankhwar S, Dalela D (2009) Antiplatelet drugs and the perioperative period: what every urologist needs to know. Indian J Urol 25:296–301
Mayor S (2006) Drug-eluting stents are safe for licensed indications, FDA panel says. BMJ 333:1235
Silber S, Albertsson P, Avilés FF et al (2005) Guidelines for percutaneous coronary interventions. The Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Eur Heart J 26:804–847
Carmignani L, Picozzi S (2009) Re: noncardiac surgery and antiplatelet therapy following coronary artery stenting. Heart 95:1537
Eisenstein EL, Anstrom KJ, Kong DF et al (2007) Clopidogrel use and long-term clinical outcomes after drug-eluting stent implantation. JAMA 297:159–168
Straus SE, Majumdar SR, McAlister FA (2002) New evidence for stroke prevention: scientific review. JAMA 288:1388–1395
Llinas RH (2006) Could discontinuation of aspirin therapy be a trigger for stroke? Nat Clin Pract Neurol 2:300–301
Cook LJ, Cottrell AM (2010) Anti-platelet agents in urology. BJU Int. www.bjui.org/FileStreaming.aspx?fileid=311
Di Minno MN, Prisco D, Ruocco AL, Mastronardi P, Massa S, Di Minno G (2009) Perioperative handling of patients on antiplatelet therapy with need for surgery. Intern Emerg Med 4:279–288
Chassot PG, Delabays A, Spahn DR (2007) Perioperative antiplatelet therapy: the case for continuing therapy in patients at risk of myocardial infarction. Br J Anaesth 99:316–328
Samama CM, Bastien O, Forestier F et al (2002) Antiplatelet agents in the perioperative period: expert recommendations of the French Society of Anesthesiology and Intensive Care (SFAR) 2001—summary statement. Can J Anaesth 49:S26–S35
Urmey WF, Rowlingson J (1998) Do antiplatelet agents contribute to the development of perioperative spinal hematoma? Reg Anesth Pain Med 23:146–151
Horlocker TT, Wedel DJ, Benzon H et al (2003) Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg Anesth Pain Med 28:172–197
Horlocker TT, Wedel DJ, Rowlingson JC et al (2010) Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (third edition). Reg Anesth Pain Med 35:64–101
Eagle KA, Rihal CS, Mickel MC, Holmes DR, Foster ED, Gersh BJ (1997) Cardiac risk of noncardiac surgery: influence of coronary disease and type of surgery in 3368 operations. CASS Investigators and University of Michigan Heart Care Program. Coronary Artery Surgery Study. Circulation 96:1882–1887
Eagle RA, Berger PB, Calkins H et al (2002) ACC/AHA Guideline Update for Perioperative Cardiovascular Evaluation for Noncardiac Surgery—Executive Summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Anesth Analg 94:1052–1064
de Korte FI, van Werkum JW, Vijverberg PL, Ten Berg JM (2008) Late coronary stent thrombosis complicating urologic surgery. Eur Urol 54:221–225
Carmignani L, Picozzi S, Stubinski R et al (2011) Endoscopic resection of bladder cancer in patients receiving double platelet antiaggregant therapy. Surg Endosc 25:2281–2287
Ehrlich Y, Yossepowitch O, Margel D, Lask D, Livne PM, Baniel J (2007) Early initiation of aspirin after prostate and transurethral bladder surgeries is not associated with increased incidence of postoperative bleeding: a prospective, randomized trial. J Urol 178:524–528
Disclosures
Stefano Picozzi, Carlo Marenghi, Cristian Ricci, Giorgio Bozzini, Stefano Casellato, and Luca Carmignani have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Picozzi, S., Marenghi, C., Ricci, C. et al. Risks and complications of transurethral resection of bladder tumor among patients taking antiplatelet agents for cardiovascular disease. Surg Endosc 28, 116–121 (2014). https://doi.org/10.1007/s00464-013-3136-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3136-8