
Abstract
Background
Percutaneous endoscopic gastrostomy (PEG) remains a mainstay of enteral access. Thirty-day mortality for PEG has ranged from 16 to 43 %. This study aims to discern patient groups that demonstrate limited survival after PEG placement. The Enterprise Data Warehouse (EDW) concept allows an efficient means of integrating administrative, clinical, and quality-of-life data. On the basis of this concept, we developed the Vanderbilt Procedural Outcomes Database (VPOD) and analyzed these data for evaluation of post-PEG mortality over time.
Methods
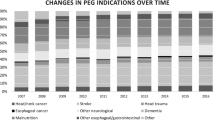
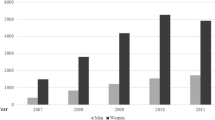
Patients were identified using the VPOD from 2008 to 2010 and followed for 1 year after the procedure. Patients were categorized according to common clinical groups for PEG placement: stroke/CNS tumors, neuromuscular disorders, head and neck cancers, other malignancies, trauma, cerebral palsy, gastroparesis, or other indications for PEG. All-cause mortality at 30, 60, 90, 180, and 360 days was determined by linking VPOD information with the Social Security Death Index. Chi-square analysis was used to determine significance across groups.
Results
Nine hundred fifty-three patients underwent PEG placement during the study period. Mortality over time (30-, 60-, 90-, 180-, and 360-day mortality) was greatest for patients with malignancies other than head and neck cancer (29, 45, 57, 66, and 72 %) and least for cerebral palsy or patients with gastroparesis (7 % at all time points). Patients with neuromuscular disorders had a similar mortality curve as head and neck cancer patients. Stroke/CNS tumor patients and patients with other indications had the second highest mortality, while trauma patients had low mortality.
Conclusions
PEG mortality was much higher in patients with malignancies other than head and neck cancer compared to previously published rates. PEG should be used with great caution in this and other high-risk patient groups. This study demonstrates the power of an EDW-based database to evaluate large numbers of patients with clinically meaningful results.

Similar content being viewed by others

References
Gauderer MW, Ponsky JL, Izant RJ Jr (1980) Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg 15:872–875
Bin Basri H (2006) Predicting the outcome of percutaneous endoscopic gastrostomy tube feeding. Singapore Med J 47:1013
Johnston SD, Tham TCK, Mason M (2008) Death after PEG: results of the National Confidential Enquiry into Patient Outcome and Death. Gastrointest Endosc 68:223–227
Rustom IK, Jebreel A, Tayyab M, England RJA, Stafford ND (2006) Percutaneous endoscopic, radiological and surgical gastrostomy tubes: a comparison study in head and neck cancer patients. J Laryngol Otol 120:463–466
Hoskins K, Dahodwala N, Elman L, Golaszewski A, Palovcak M, McCluskey L (2010) Beliefs around percutaneous endoscopic gastrostomy tube placement in ALS patients. Amyotroph Lateral Scler 11:136
Leeds JS, McAlindon ME, Grant J, Robson HE, Lee FK, Sanders DS (2010) Survival analysis after gastrostomy: a single-centre, observational study comparing radiological and endoscopic insertion. Eur J Gastroenterol Hepatol 22:591–596
Longcroft-Wheaton G, Marden P, Colleypriest B, Gavin D, Taylor G, Farrant M (2009) Understanding why patients die after gastrostomy tube insertion: a retrospective analysis of mortality. JPEN J Parenter Enteral Nutr 33:375–379
Dwyer KM, Watts DD, Thurber JS, Benoit RS, Fakhry SM (2002) Percutaneous endoscopic gastrostomy: the preferred method of elective feeding tube placement in trauma patients. J Trauma 52:26–32
Disclosures
Dr. Poulose has received research support from Karl Storz Endoscopy unrelated to contents of this article. Mrs. Kaiser and Drs. Beck, Jackson, Nealon, Sharp, and Holzman have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Poulose, B.K., Kaiser, J., Beck, W.C. et al. Disease-based mortality after percutaneous endoscopic gastrostomy: utility of the enterprise data warehouse. Surg Endosc 27, 4119–4123 (2013). https://doi.org/10.1007/s00464-013-3077-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-3077-2