
Abstract
Background
Laparoscopic intestinal surgery is the preferable technique for the majority of intestinal surgical disorders. However, no series on laparoscopic resection of intestinal midgut carcinoid tumors (MCTs) has been reported to date. This is related to the rarity of these tumors as well as the technical difficulties resecting the large mesenteric root lymph node mass commonly found with these tumors and the occasional difficulty identifying the primary MCT, which may be small and undetected on preoperative imaging studies. This is the first series to report the results for laparoscopic resection of MCT.
Methods
All consecutive patients with MCT (excluding appendiceal carcinoid tumor) between 2002 and 2012 underwent laparoscopic resection. The patient’s clinical data, preoperative endocrine workup, imaging studies, operative data, final histology, and outcome were recorded and analyzed.
Results
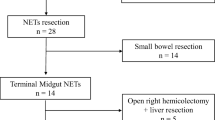
During the study period, 35 patients underwent surgery for primary intestinal carcinoid tumor. Of the 35 patients, 20 (12 women and 8 men ages 26–86 years) had surgery for primary MCT, and the remainder had a colorectal carcinoid tumor. In the MCT group, ten patients had liver metastases at the time of surgery. In three patients, multiple synchronous MCTs were detected intraoperatively. All the patients underwent a laparoscopic resection with en bloc resection of the corresponding mesenteric root mass. No conversion to open surgery was needed, and no major morbidity occurred. Two patients (10 %) each experienced minor morbidity with wound infection and prolonged ileus. The median hospital length of stay was 6 days (range 4–9 days). During a follow-up period of 3–96 months, no patients experienced local or regional recurrence. No distant metastases were detected during the follow-up period in any patients who had surgery with intent to cure.
Conclusion
Although technically difficult, laparoscopic resection of primary MCTs is feasible and safe, with the additional known significant advantages of laparoscopic surgery in general. Similar to the large-scale prospective studies that proved the oncologic safety of laparoscopic surgery for colorectal cancer, this small series showed that the laparoscopic technique also may be oncologically safe for these rare tumors.
Similar content being viewed by others


References
Perez EA, Koniaris LG, Snell SE, Gutierrez JC, Summer WE III, Lee DJ (2007) 7201 Carcinoids: increasing incidence overall and disproportionate mortality in the elderly. World J Surg 31:1022. doi:10.1007/s00268-005-0774-6
Robertson RG, Geiger WJ, Davis NB (2006) Carcinoid tumors. Am Fam Phys 74:429–434
Akerstrom G, Hellman P (2007) Surgery on neuroendocrine tumours. Best Pract Res Clin Endocrinol Metab 21:87–109
Rindi G (2010) The ENETS guidelines: the new TNM classification system. Tumori 96:806–809
Akerstrom GHP, Hessman O (2006) Gastrointestinal carcinoids. In: Lennard TWJ (ed) Endocrine surgery. Elsevier, Edinburgh
Hellman P, Lundstrom T, Ohrvall U, Eriksson B, Skogseid B, Oberg K (2002) Effect of surgery on the outcome of midgut carcinoid disease with lymph node and liver metastases. World J Surg 26:991. doi:10.1007/s00268-002-6630-z
Reissman P, Salky BA, Pfeifer J, Edye M, Jagelman DG, Wexner SD (1996) Laparoscopic surgery in the management of inflammatory bowel disease. Am J Surg 171:47–51
Reissman P, Agachan F, Wexner SD (1996) Outcome of laparoscopic colorectal surgery in older patients. Am Surg 62:1060–1063
Clinical Outcomes of Surgical Therapy Study Group (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350:2050–2059
Bonjer HJ, Hop WC, Nelson H (2007) Laparoscopically assisted vs open colectomy for colon cancer: a meta-analysis. Arch Surg 142:298–303
Jackson TD, Kaplan GG, Arena G, Page JH, Rogers SO Jr (2007) Laparoscopic versus open resection for colorectal cancer: a metaanalysis of oncologic outcomes. J Am Coll Surg 204:439–446
Sylla P, Kirman I, Whelan RL (2005) Immunological advantages of advanced laparoscopy. Surg Clin N Am 85:1–18
Veenhof AA, Vlug MS, van der Pas MH, Sietses C, van der Peet DL, de Klerk ESL (2012) Surgical stress response and postoperative immune function after laparoscopy or open surgery with fast track or standard perioperative care: a randomized trial. Ann Surg 255:216–221
Capurso G, Rinzivillo M, Bettini R, Boninsegna L, Fave GD, Falconi M (2012) Systematic review of resection of primary midgut carcinoid tumour in patients with unresectable liver metastases. Br J Surg 99:1480–1486
Maartense S, Dunker MS, Slors JF, Cuesta M, Gouma DJ, van Deventer SJ (2004) Hand-assisted laparoscopic versus open restorative proctocolectomy with ileal pouch anal anastomosis: a randomized trial. Ann Surg 240:984–991 (discussion 91–92)
Norlen O, Hessman O, Stalberg P, Akerstrom G, Hellman P (2010) Prophylactic cholecystectomy in midgut carcinoid patients. World J Surg 34:1361. doi:10.1007/s00268-010-0428-1
Disclosures
Petachia Reissman, Shmail Shmailov, Simona Grozinsky-Glasberg, and David J. Gross have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reissman, P., Shmailov, S., Grozinsky-Glasberg, S. et al. Laparoscopic resection of primary midgut carcinoid tumors. Surg Endosc 27, 3678–3682 (2013). https://doi.org/10.1007/s00464-013-2944-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-013-2944-1