
Abstract
Background
Laparoscopic ventral rectopexy (LVR) is an established technique for the treatment of rectal prolapse. Several techniques and devices can be used for proximal mesh fixation on the sacral promontory during this procedure. The aim of this study was to compare the fixation strength of a recently introduced screw for mesh fixation on the promontory during LVR with two other frequently used techniques.
Methods
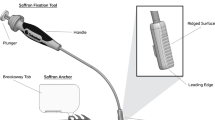
An ex vivo experimental model using a porcine spinal column was designed to measure the strength of proximal mesh fixation. In a laparoscopic box trainer, a polypropylene mesh was anchored on the spinal column using three different fixation methods, i.e., the Protack 5-mm tacker device, Ethibond Excel 2-0 stitches, and the Karl Storz screw. Subsequently, increasing traction was applied to the mesh. This traction was applied at a standardized angle as determined by measuring the mean angle between the site of distal mesh fixation on the rectum and a line straight through the sacral promontory on 12 random dynamic MR scans of the pelvic floor after the LVR procedure. The applied force was measured at the moment that the fixation broke, using a calibrated electronic Newton meter. All fixation methods were tested ten times.
Results
The mean angle, as measured on the MR scans, was 100°. The mean disruption force, which led to a break of the proximal mesh fixation, was 58 N for the three Protack tacks, 55 N for the two stitches, and 70 N for the new screw. The use of a screw therefore led to a significantly stronger fixation compared to the use of stitches (p ≤ 0.05). No significant difference was determined between the tacks and the screw fixation and between the tacks and the stitches fixation.
Conclusion
The new screw for proximal mesh fixation during LVR procedures offers similar fixation strength when compared to tacks. The use of one screw for proximal mesh fixation is therefore a reasonable alternative to the use of several tacks or sutures.



Similar content being viewed by others


References
Wu JS (2009) Rectal prolapse: a historical perspective. Curr Probl Surg 46(8):602–716
Wijffels NA, Collinson R, Cunningham C, Lindsey I (2010) What is the natural history of internal rectal prolapse? Colorectal Dis 12(8):822–830
Madiba TE, Baig MK, Wexner SD (2005) Surgical management of rectal prolapse. Arch Surg 140(1):63–73
Boons P, Collinson R, Cunningham C, Lindsey I (2010) Laparoscopic ventral rectopexy for external rectal prolapse improves constipation and avoids de novo constipation. Colorectal Dis 12(6):526–532
Collinson R, Wijffels N, Cunningham C, Lindsey I (2010) Laparoscopic ventral rectopexy for internal rectal prolapse: short-term functional results. Colorectal Dis 12(2):97–104
D’Hoore A, Cadoni R, Penninckx F (2004) Long-term outcome of laparoscopic ventral rectopexy for total rectal prolapse. Br J Surg 91(11):1500–1505
D’Hoore A, Penninckx F (2006) Laparoscopic ventral recto(colpo)pexy for rectal prolapse: surgical technique and outcome for 109 patients. Surg Endosc 20(12):1919–1923
Slawik S, Soulsby R, Carter H, Payne H, Dixon AR (2008) Laparoscopic ventral rectopexy, posterior colporrhaphy and vaginal sacrocolpopexy for the treatment of recto-genital prolapse and mechanical outlet obstruction. Colorectal Dis 10(2):138–143
van den Esschert JW, van Geloven AA, Vermulst N, Groenedijk AG, de Wit LT, Gerhards MF (2008) Laparoscopic ventral rectopexy for obstructed defecation syndrome. Surg Endosc 22(12):2728–2732
Wijffels N, Cunningham C, Dixon A, Greenslade G, Lindsey I (2011) Laparoscopic ventral rectopexy for external rectal prolapse is safe and effective in the elderly. Does this make perineal procedures obsolete? Colorectal Dis 13(5):561–566
Cobb WS, Burns JM, Kercher KW, Matthews BD, James NH, Todd HB (2005) Normal intra-abdominal pressure in healthy adults. J Surg Res 129(2):231–235
Disclosure
Drs. Formijne Jonkers, Draaisma, Heggelman, Consten, and Broeders and Mr. Van de Haar have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Formijne Jonkers, H.A., van de Haar, H.J., Draaisma, W.A. et al. The optimal strategy for proximal mesh fixation during laparoscopic ventral rectopexy for rectal prolapse: an ex vivo study. Surg Endosc 26, 2208–2212 (2012). https://doi.org/10.1007/s00464-012-2161-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2161-3