
Abstract
Background
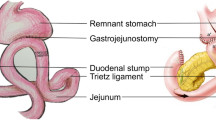
We performed this prospective randomized study to evaluate what is the best reconstruction method after distal gastrectomy for gastric cancer.
Methods
One hundred fifty-nine patients who underwent laparoscopy-assisted or open gastrectomy for gastric cancer were analyzed from March 2006 to August 2007. Billroth I (B-I) anastomosis, Billroth II (B-II) with Braun anastomosis, and Roux-en-Y (R-Y) anastomosis were applied randomly. Additionally, the patients were divided into two groups based on treatment type: laparoscopic and open operation. Endoscopy and hepatobiliary scans were performed to investigate gastric stasis and enterogastric reflux. The Gastrointestinal Quality of Life Index (GIQLI) was used to evaluate postoperative quality of life, and the hematologic test was used to assess nutritional aspect.
Results
Endoscopy revealed that reflux after the R-Y anastomosis procedure was significantly less frequent than after the other anastomosis types at 12 months. Comparison of the GIQLI and the nutritional parameters between the reconstruction types revealed that there were no differences, but a significantly higher GIQLI score was observed in the laparoscopic group immediately following the procedure (P = 0.042).
Conclusions
R-Y anastomosis is superior to B-I and B-II with Braun anastomosis in terms of frequency of bile reflux, despite the fact that there is no difference in the postoperative quality-of-life index and nutritional status between reconstructive procedures. The laparoscopic approach is the better option than open surgery in terms of QOL in the immediate postoperative period.


Similar content being viewed by others


References
Nakajima T (2002) Gastric cancer treatment guidelines in Japan. Gastric Cancer 5(1):1–5
Lee SI, Choi YS, Park DJ, Kim HH, Yang HK, Kim MC (2006) Comparative study of laparoscopy-assisted distal gastrectomy and open distal gastrectomy. J Am Coll Surg 202(6):874–880
Svensson JO (1983) Duodenogastric reflux after gastric surgery. Scand J Gastroenterol 18(6):729–734
Japanese Gastric Cancer Association (1998) Japanese classification of gastric carcinoma–2nd English edn. Gastric Cancer 1(1):10–24
Kubo M, Sasako M, Gotoda T, Ono H, Fujishiro M, Saito D, Sano T, Katai H (2002) Endoscopic evaluation of the remnant stomach after gastrectomy: proposal for a new classification. Gastric Cancer 5(2):83–89
Miwa H, Yokoyama T, Hori K, Sakagami T, Oshima T, Tomita T, Fujiwara Y, Saita H, Oqawa H, Nakamura Y, Kishi K, Murayama Y, Hayashi E, Kobayashi K, Tano N, Matsushita K, Kawamoto H, Sawada Y, Ohkawa A, Arai E, Nagao K, Hamamoto N, Sugiyasu Y, Sugimoto K, Hara H, Tanimura M, Honda Y, Isozaki K, Noda S, Kubota S, Himeno S (2008) Interobserver agreement in endoscopic evaluation of reflux esophagitis using a modified Los Angeles classification incorporating grades N and M: a validation study in a cohort of Japanese endoscopists. Dis Esophagus 21(4):355–363
Eypasch E, Williams JI, Wood-Dauphinee S, Ure BM, Schmulling C, Neugebauer E, Troidl H (1995) Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. Br J Surg 82(2):216–222
Osugi H, Fukuhara K, Takada N, Takemura M, Kinoshita H (2004) Reconstructive procedure after distal gastrectomy to prevent remnant gastritis. Hepatogastroenterology 51(58):1215–1218
Sato T, Miwa K, Sahara H, Segawa M, Hattori T (2002) The sequential model of Barrett’s esophagus and adenocarcinoma induced by duodeno-esophageal reflux without exogenous carcinogens. Anticancer Res 22(1A):39–44
Werscher GJ, Hinder RA, Smyrk T, Perdikis G, Adrian TE, Profanter C (1999) Gastric acid blockade with omeprazole promotes gastric carcinogenesis induced by duodenogastric reflux. Dig Dis Sci 44(6):1132–1135
Goldstein SR, Yang GY, Curtis SK, Reuhl KR, Liu BC, Mirvish SS, Newmark HL, Yang CS (1997) Development of esophageal metaplasia and adenocarcinoma in rat surgical model without the use of a carcinogen. Carcinogenesis 18(11):2265–2270
Lillimoe KP, Johnson LF, Harmon JW (1982) Role of the components of the gastroduodenal contents in experimental acid esophagitis. Surgery 92(2):276–284
Shinoto K, Ochiai T, Suzuki T, Okazumi S, Ozaki M (2003) Effectiveness of Roux-en-Y reconstruction after distal gastrectomy based on an assessment of biliary kinetics. Surg Today 33(3):169–177
Vogel SB, Drane WE, Woodwar ER (1994) Clinical and radionuclide evaluation of bile diversion by Braun enteroenterostomy: prevention and treatment of alkine reflux gastritis. an alternative to Roux-en-Y diversion. Ann Surg 219(5):458–465
Chan DC, Fan YM, Lin CK, Chen CJ, Chao YC (2007) Roux-en-Y reconstruction after distal gastrectomy to reduce enterogastric reflux and Helicobacter pylori infection. J Gastrointest Surg 11(12):1732–1740
Fukuhara K, Osugi H, Takada N, Takemura M, Higashino M, Kinoshita H (2002) Reconstructive procedure after distal gastrectomy for gastric cancer that best prevents duodenogastroesophagel reflux. World J Surg 26(12):1452–1457
Kojima K, Yamada H, Inokuchi M, Kawano T, Sugihara K (2008) A comparison of Roux-en-Y and Billroth-I reconstruction after laparoscopy-assisted distal gastrectomy. Ann Surg 247(6):962–967
Hoya Y, Mitsumori N, Yanaga K (2009) The advantages and disadvantages of a Roux-en-Y reconstruction after a distal gastrectomy for gastric cancer. Surg Today 39(8):647–651
Namikawa T, Kitagawa H, Okabayashi T, Sugimoto T, Kobayashi M, Hanazaki K (2010) Roux-en-Y reconstruction is superior to Billroth I reconstruction in reducing reflux esophagitis after distal gastrectomy: special relationship with the angle of His. World J Surg 34(5):1022–1027
Gustavsson S, Ilstrup DM, Morrison P, Kelly KA (1988) Roux-Y stasis syndrome after gastrectomy. Am J Surg 155(3):490–494
Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H (1997) Endoscopic access to the papilla of Vater for endoscopic retrograde cholangiopancreatography in patients with Billroth II or Roux-en-Y gastrojejunostomy. Endoscopy 29(2):69–73
Iwamoto S, Ryozawa S, Yamamoto H, Taba K, Ishigaki N, Harano M, Iwano H, Sakaida I (2010) Double balloon endoscope facilitates endoscopic retrograde cholangiopancreatography in Roux-en-Y anastomosis patients. Dig Endosc 22(1):64–68
Kim BJ, O’Connell T (1999) Gastroduodenostomy after gastric resection for cancer. Am Surg 65(10):905–907
Montesani C, D’Amato A, Santella S, Pronio A, Giovannini C, Cristaldi M, Ribotta G (2002) Billroth I versus Billroth II versus Roux-en-Y after subtotal gastrectomy. Prospective randomized study. Hepatogastroenterology 49(47):1469–1473
Johnsson F, Joelsson B, Gudmundsson K, Greiff L (1987) Symptoms and endoscopic findings in the diagnosis of gastroesophageal reflux disease. Scand J Gastroenterol 22(6):714–718
Shiraishi N, Yasuda K, Kitano S (2006) Laparoscopic gastrectomy with lymph node dissection for gastric cancer. Gastric Cancer 9(3):167–176
Kitagawa Y, Kitano S, Kubota T, Kumai K, Otani Y, Saikawa Y, Yoshida M, Kitajima M (2005) Minimally invasive surgery for gastric cancer–toward a confluence of two major streams: a review. Gastric Cancer 8(2):103–110
Acknowledgment
This study was supported by grant 02-2006-021 from Seoul National University Bundang Hospital, Republic of Korea.
Disclosures
M.-S. Lee, S.-H. Ahn, J.-H. Lee, D. J. Park, H.-J. Lee, H.-H. Kim, H.-K. Yang, Nayoung Kim, and W. W. Lee have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
This clinical trial was not registered in a public acceptable trials registry.
Rights and permissions
About this article
Cite this article
Lee, MS., Ahn, SH., Lee, JH. et al. What is the best reconstruction method after distal gastrectomy for gastric cancer?. Surg Endosc 26, 1539–1547 (2012). https://doi.org/10.1007/s00464-011-2064-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-2064-8