
Abstract
Background
Common video systems for laparoscopy provide the surgeon a two-dimensional image (2D), where information on spatial depth can be derived only from secondary spatial depth cues and experience. Although the advantage of stereoscopy for surgical task efficiency has been clearly shown, several attempts to introduce three-dimensional (3D) video systems into clinical routine have failed. The aim of this study is to evaluate users’ performances in standardised surgical phantom model tasks using 3D HD visualisation compared with 2D HD regarding precision and working speed.
Methods
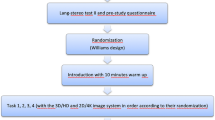
This comparative study uses a 3D HD video system consisting of a dual-channel laparoscope, a stereoscopic camera, a camera controller with two separate outputs and a wavelength multiplex stereoscopic monitor. Each of 20 medical students and 10 laparoscopically experienced surgeons (more than 100 laparoscopic cholecystectomies each) pre-selected in a stereo vision test were asked to perform one task to familiarise themselves with the system and subsequently a set of five standardised tasks encountered in typical surgical procedures. The tasks were performed under either 3D or 2D conditions at random choice and subsequently repeated under the other vision condition. Predefined errors were counted, and time needed was measured.
Results
In four of the five tasks the study participants made fewer mistakes in 3D than in 2D vision. In four of the tasks they needed significantly more time in the 2D mode. Both the student group and the surgeon group showed similarly improved performance, while the surgeon group additionally saved more time on difficult tasks.
Conclusions
This study shows that 3D HD using a state-of-the-art 3D monitor permits superior task efficiency, even as compared with the latest 2D HD video systems.



Similar content being viewed by others


References
Matouschek E, Becker H (1995) The value of 3D video endoscopy for surgical procedures. Bildgebung 62:174–178
Buess GF, van Bergen P, Kunert W, Schurr MO (1996) Comparative study of various 2-D and 3-D vision systems in minimally invasive surgery. Chirurg 67:1041–1046
van Bergen P, Kunert W, Bessell J, Buess GF (1998) Comparative study of two-dimensional and three-dimensional vision systems for minimally invasive surgery. Surg Endosc 12:948–954
LaGrange CA, Clark CJ, Gerber EW, Strup SE (2008) Evaluation of three laparoscopic modalities: robotics versus three-dimensional vision laparoscopy versus standard laparoscopy. J Endourol 22:511–516
Taffinder N, Smith SG, Huber J, Russell RC, Darzi A (1999) The effect of a second-generation 3D endoscope on the laparoscopic precision of novices and experienced surgeons. Surg Endosc 13:1087–1092
Kong SH, Oh BM, Yoon H, Ahn HS, Lee HJ, Chung SG, Shiraishi N, Kitano S, Yang HK (2010) Comparison of two- and three-dimensional camera systems in laparoscopic performance: a novel 3D system with one camera. Surg Endosc 24:1132–1143
Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS (2006) Impact of 2D and 3D vision on performance of novice subjects using da Vinci robotic system. Acta Chir Belg 106:662–664
van Bergen P, Kunert W, Buess GF (2000) The effect of high-definition imaging on surgical task efficiency in minimally invasive surgery: an experimental comparison between three-dimensional imaging and direct vision through a stereoscopic TEM rectoscope. Surg Endosc 14:71–74
Shah J, Buckley D, Frisby J, Darzi A (2003) Depth cue reliance in surgeons and medical students. Surg Endosc 17:1472–1474
Brigner WL, Deni JR, Hildreth LL (1994) Simultaneous changes in length and direction as a cue for perceived depth. Percept Mot Skills 78:1385–1386
Mather G, Smith DR (2000) Depth cue integration: stereopsis and image blur. Vis Res 40:3501–3506
O’Shea RP, Blackburn SG, Ono H (1994) Contrast as a depth cue. Vis Res 34:1595–1604
Rogers B (2009) Motion parallax as an independent cue for depth perception: a retrospective. Perception 38:907–911
Voorhorst FA, Overbeeke KJ, Smets GJ (1996) Using movement parallax for 3D laparoscopy. Med Prog Technol 21:211–218
Arezzo A, Kees T, Kunert W, De Gregori M, Buess G (2000) Shadow optic. An endoscope with optimized light. Chir Ital 52:451–453
Buess G, Theiss R, Gunther M, Hutterer F, Pichlmaier H (1985) Endoscopic surgery in the rectum. Endoscopy 17:31–35
Muller-Richter UD, Limberger A, Weber P, Schilling M (2003) Comparative study of spatial imaging techniques in stereo-endoscopy. Mund Kiefer Gesichtschir 7:157–163
Inoue H, Tanaka H (1967) Relationship between abdnormal position of the eye and amblyopia, and angle of stereopsis for near object—mainly about the results due to stereotests. Nippon Ganka Gakkai Zasshi 71:92–97
Julesz B (1964) Binocular depth perception without familiarity cues. Science 145:356–362
Acknowledgments
The 3D HD TV project was funded by the German Federal Ministry of Economics and Technology. The stereoscopic laparoscope with the 6CCD endocam was a purpose-built item devised by Richard Wolf GmbH, Knittlingen, Germany. The 3D wavelength multiplex monitor is patented and constructed by INFITEC GmbH, Ulm, Germany.
Disclosures
Authors P. Storz, W. Kunert, G.F. Buess and A. Kirschniak have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Gerhard F. Buess—deceased.
Rights and permissions
About this article
Cite this article
Storz, P., Buess, G.F., Kunert, W. et al. 3D HD versus 2D HD: surgical task efficiency in standardised phantom tasks. Surg Endosc 26, 1454–1460 (2012). https://doi.org/10.1007/s00464-011-2055-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-2055-9