
Abstract
Background
Although the efficacy and safety of extensive endomucosal resection (EMR) in eradicating Barrett’s esophagus (BE) harbouring early neoplasia have been established, factors predicting efficacy remains unclear.
Aim
To determine the complete eradication rate of Barrett’s esophagus with high-grade intraepithelial neoplasia (HGIN) or intramucosal carcinoma (IMC), safety, and factors predicting complete eradication by EMR.
Methods
Patients with histological confirmation of Barrett’s HGIN/IMC were prospectively identified. EMR was performed using Duette multiband ligator or cap technique by a single operator (NEM).
Results
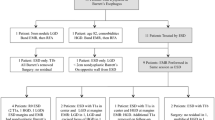
99 patients (81 males) with median age 67 years [interquartile range (IQR) 60–77 years] and median Barrett’s length 4 cm (IQR 2–6 cm) were included. Of 628 index EMRs [mean 6.3, median 5 (IQR 3–8)], 23% showed IMC, 58.5% showed HGIN, and 16% showed low-grade dysplasia only. A median of 8 EMR resections per patient (IQR 6–16, 1,064 resections in 89 patients) resulted in complete eradication of BE harboring neoplasia in 49.4% and eradication of HGIN/IMC in 81% (BE <5 cm subgroup: 65% complete eradication and 91% HGIN eradication) at median follow-up of 18 months (range 6–27 months). On univariate analysis, focal dysplasia (P = 0.003) and Barrett’s length <5 cm (P = 0.001) were predictors of complete BE eradication. Barrett’s length <5 cm was the only significant predictor [odds ratio (OR) 3.4, standard error (SE) 0.11, P = 0.0006] on multiple logistic regression analysis. Strictures developed in 27% and major bleeding in 2% with no procedure-related perforations or mortality.
Conclusions
Extensive EMR for removal of BE with early neoplasia is safe. Outcomes for complete BE eradication are modest at 49.4% and eradication of high-grade dysplasia at 81%. Barrett’s length <5 cm is the only significant predictor of complete response.

Similar content being viewed by others

References
Ferguson MK, Martin TR, Reeder LB et al (1997) Mortality after oesophagectomy: risk factor analysis. World J Surg 21(6):599–603
Reavis KM, Smith BR, Hinojosa MW, Nguyen NT (2008) Outcomes of esophagectomy at academic centers: an association between volume and outcome. Ann Surg 74(10):939–943
Nguyen NT, Hinojosa MW, Smith BR et al (2008) Minimally invasive oesophagectomy: lessons learnt from 104 operations. Ann Surg 248:1081–1091
Overholt BF, Wang KK, Burdick JS et al (2007) Five-year efficacy and safety of photodynamic therapy with Photofrin in Barrett’s high-grade dysplasia. Gastrointest Endosc 66:460–468
Barr H, Shepherd NA, Dix A et al (1996) Eradication of high-grade dysplasia in columnar lined (Barrett’s) oesophagus by photodynamic therapy by endogenously generated protoporphyrin IX. Lancet 348:584–585
Overholt BF, Panjehpour M, Heydek JM et al (1999) Photodynamic therapy for Barrett’s oesophagus: follow up in 100 patients. Gastrintest Endosc 49:1–7
Shaheen NJ, Sharma P, Overholt BF et al (2009) Radiofrequency ablation in Barrett’s esophagus with dysplasia. N Eng J Med 360:2277–2288
Gondrie JJ, Pouw RE, Sondermeijer CM et al (2008) Effective treatment of early Barrett’s neoplasia with stepwise circumferential and focal ablation using the HALO system. Endoscopy 40:370–379
Seewald S, Akaraviputh T, Seitz U et al (2003) Circumferential EMR and complete removal of Barrett’s epithelium: a new approach to the management of Barrett’s esophagus containing high-grade intraepithelial neoplasia and intramucosal carcinoma. Gastrointest Endosc 57:854–859
Giovannini M, Bories E, Pesenti C et al (2004) Circumferential endoscopic mucosal resection in Barrett’s esophagus with high-grade intraepithelial neoplasia or mucosal cancer. Preliminary results in 21 patients. Endoscopy 36:782–787
Peters FP, Kara MA, Rosmolen WD et al (2006) Stepwise radial endoscopic resection is effective for complete removal, of Barrett’s oesophagus with early neoplasia. Am J Gastroenterol 101:1449–1457
Larghi A, Lightdale CJ, Ross AS et al (2007) Long-term follow up of complete Barrett’s eradication endoscopic mucosal resection for the treatment of high-grade dysplasia and intramucosal carcinoma. Endoscopy 39:1086–1091
Inoue H, Takeshita K, Hori H et al (1993) Endoscopic mucosal resection with a cap fitted panendoscope for esophagus, stomach and colon mucosal lesions. Gastrointest Endosc 39:58–62
Soehendra N, Binmoeller KF, Bohnacker S et al (1997) Endoscopic snare mucosectomy in the oesophagus without any additional equipment: a simple technique of resecting flat early cancer. Endoscopy 29:380–383
Schlempler RJ, Riddell RH, Kato Y et al (2000) The Vienna classification of gastrointestinal epithelial neoplasia. Gut 47:251–255
Nijhawan PK, Wang KK (2000) Endoscopic mucosal resection for lesions with endoscopic features suggestive of malignancy and high-grade dysplasia within Barrett’s oesophagus. Gastrointest Endosc 52:328–332
Buttar NS, Wang KK, Lutzke LS et al (2001) Combined endoscopic mucosal resection and photodynamic therapy for oesophageal neoplasia within Barrett’s oesophagus. Gastrointest Endosc 54:682–688
Pech O, Behrens A, May A et al (2008) Long-term results and risk factor analysis for recurrence after curative endoscopic therapy in 349 patients with high-grade intraepithelial neoplasia and mucosal adenocarcinoma in Barrett’s oesophagus. Gut 57:1200–1206
May A, Gossner L, Pech O et al (2002) Local endoscopic therapy for intraepithelial high-grade neoplasia and early adenocarcinoma in Barrett’s oesophagus: acute phase and intermediate results of a new treatment approach. Eur J Gastroenterol Hepatol 14:1085–1091
Ell C, May A, Gossner L et al (2000) Endoscopic mucosal resection of early cancer and high-grade dysplasia in Barrett’s oesophagus. Gastroenterology 118:670–677
Pouw RE, Peters FB, Curvers LW et al (2007) Stepwise radial endoscopic resection for complete removal, of Barrett’s oesophagus with early neoplasia. A prospective study of 56 patients with 2 years follow up. Gastrointest Endosc 65:AB133 (Abstract)
Gondrie JJ, Seewald S, Pouw ER et al (2008) Stepwise radical endoscopic resection for complete removal of Barrett’s esophagus with early neoplasia: international multicentre study. Gastrointest Endosc 67:AB175–AB176 (Abstract)
Ormsby AH, Kilqore SP, Goldblum JR et al (2000) The location and frequency of intestinal metaplasia at the esophagogastric junction in 223 consecutive autopsies. Implications for patient treatment and preventive strategies in Barrett’s oesophagus. Mod Pathol 13:614–620
Yachimski P, Puricelli WP, Nishioka NS (2008) Patient predictors of histopathologic response after photodynamic therapy of Barrett’s esophagus with high-grade dysplasia or intramucosal carcinoma. Gastrointst Endosc 69(2):205–212
Kerkhof M, Van Dekken H, Steyerberg EW et al (2007) Grading of dysplasia in Barrett’s oesophagus: substantial interobserver variation between general and gastrointestinal pathologists. Histopathology 50:920–927
Levine DS, Haggitt RC, Blount PL et al (1993) An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s oesophagus. Gastroenterology 105:40–50
Katada C, Muto M, Manabe T et al (2003) Esophageal stenosis after endoscopic mucosal resection of superficial oesophageal lesions. Gastrointest Endosc 57:165–169
Pech O, May A, Gunter E et al (2006) The impact of endscopic ultrasound and computerised tomography on the TNM staging of early cancer in Barrett’s oesophagus. Am J Gastroenterol 101:2223–2229
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Thomas, T., Ayaru, L., Lee, E.Y. et al. Length of Barrett’s segment predicts success of extensive endomucosal resection for eradication of Barrett’s esophagus with early neoplasia. Surg Endosc 25, 3627–3635 (2011). https://doi.org/10.1007/s00464-011-1769-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1769-z