
Abstract
Background
Laparoscopic adrenalectomy (LA) has become the standard approach to an adrenal mass. This technique provides for decreased convalescence, less postoperative pain, and improved cosmesis. The use of LA for pheochromocytoma (PHE) has been questioned due to concerns of increased morbidity and negative hemodynamic sequelae. This study aimed to compare the outcomes of LA for PHE with the results of LA for other adrenal pathologies.
Methods
A retrospective chart review was performed for an 11-year period from July 1997 to December 2008. Patient demographics, perioperative data, and outcomes were recorded. Statistical analysis was performed using SPSS 16.0. Statistical significance was defined as a p value less than 0.05.
Results
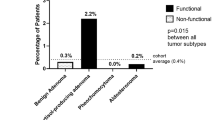
A total of 102 LA procedures were completed for 95 patients. The data for 33 PHE cases were compared with the data for 69 non-PHE cases (26 adenomas, 14 aldosteronomas, 5 cortisol-secreting tumors, 5 multinodular hyperplasias, and 19 other disorders). Five LA procedures were converted to open surgery. Four of these conversions involved patients with PHE (p = 0.03). There was no difference in the mean estimated blood loss (p = 0.2) or operative time (p = 0.1) between the two groups. The frequency of intraoperative hypertension and hypotension did not differ between the PHE and non-PHE cohorts. The complication rate was 7.5% for the PHE group and 6.9% for the non-PHE group (p = 0.7). The patients with PHE had a longer postoperative hospital stay (3.6 vs 2.3 days; p < 0.001) and overall hospital stay (4.9 vs 2.6 days; p < 0.001). Time in the intensive care unit (1.1 vs 0.1 days; p < 0.001) and time until oral intake (1.5 vs 1.0 days; p = 0.02) also were increased in the PHE population. There was one death in the PHE group secondary to congestive heart failure.
Conclusions
Concerns of increased morbidity related to a laparoscopic approach for patients with a diagnosis of PHE are unfounded. In this series, the only disparity in outcomes between the two groups was an increased conversion rate with PHE.
Similar content being viewed by others


References
Semm K (1983) Endoscopic appendectomy. Endoscopy 15:59–64
Smith CD, Weber CJ, Amerson JR (1999) Laparoscopic adrenalectomy: new gold standard. World J Surg 23:389–396
Gagner M, Breton G, Pharand D, Pomp A (1996) Is laparoscopic adrenalectomy indicated for pheochromocytomas? Surgery 120:1076–1079 (discussion 1079–1080)
Kercher KW, Novitsky YW, Park A, Matthews BD, Litwin DE, Heniford BT (2005) Laparoscopic curative resection of pheochromocytomas. Ann Surg 241:919–926 (discussion 926–928)
Humphrey R, Gray D, Pautler S, Davies W (2008) Laparoscopic compared with open adrenalectomy for resection of pheochromocytoma: a review of 47 cases. Can J Surg 51:276–280
Chan JE, Meneghetti AT, Meloche RM, Panton ON (2006) Prospective comparison of early and late experience with laparoscopic adrenalectomy. Am J Surg 191:682–686
Cheah WK, Clark OH, Horn JK, Siperstein AE, Duh QY (2002) Laparoscopic adrenalectomy for pheochromocytoma. World J Surg 26:1048–1051
Kim AW, Quiros RM, Maxhimer JB, El-Ganzouri AR, Prinz RA (2004) Outcome of laparoscopic adrenalectomy for pheochromocytomas vs aldosteronomas. Arch Surg 139:526–529 (discussion 529–531)
Chin EH, Baril DT, Weber KJ, Divino CM (2008) Laparoscopic cortical-sparing adrenalectomy for bilateral pheochromocytoma. Surg Endosc 22:2075
Tiberio GA, Baiochi GL, Arru L, Agabiti Rosei C, De Ponti S, Matheis A, Rizoni D, Giulini SM (2008) Prospective randomized comparison of laparoscopic versus open adrenalectomy for sporadic pheochromocytoma. Surg Endosc 22:1435–1439
Zacharias M, Haese A, Jurczok A, Stolzenburg JU, Fornara P (2006) Transperitoneal laparoscopic adrenalectomy: outline of the preoperative management, surgical approach, and outcome. Eur Urol 49:448–459
Fernandez-Cruz L, Saenz A, Taura P, Sabaer L, Astudillo E, Fontanais J (1998) Helium and carbon dioxide pneumoperitoneum in patients with pheochromocytoma undergoing laparoscopic adrenalectomy. World J Surg 22:1250–1255
Flavio Rocha M, Faramarzi-Roques R, Tauzin-Fin P, Vallee V, Leitao de Vasconcelos PR, Ballanger P (2004) Laparoscopic surgery for pheochromocytoma. Eur Urol 45:226–232
Li ML, Fitzgerald PA, Price DC, Norton JA (2001) Iatrogenic pheochromocytomatosis: a previously unreported result of laparoscopic adrenalectomy. Surgery 130:1072–1077
Thomson BN, Moulton CA, Davies M, Banting SW (2004) Laparoscopic adrenalectomy for phaeochromocytoma: with caution. ANZ J Surg 74:429–433
Toniato A, Boschin I, Bernante P, Opocher G, Guolo AM, Pelizzo MR, Mantero F (2007) Laparoscopic adrenalectomy for pheochromocytoma: is it really more difficult? Surg Endosc 21:1323–1326
Kalady MF, McKinlay R, Olson JA, Pinheiro J, Lagoo S, Park A, Eubanks WS (2004) Laparoscopic adrenalectomy for pheochromocytoma: a comparison to aldosteronoma and incidentaloma. Surg Endosc 18:621–625
Tatsugami K, Eto M, Hamaguci M, Yokomizo A, Harano M, Naito S (2009) What affects the results of a laparoscopic adrenalectomy for pheochromocytoma? Evaluation with respect to intraoperative blood pressure and state of tumor. J Endourol 23:101–105
Gotoh M, Ono Y, Hattori R, Kinukawa T, Onshima S (2002) Laparoscopic adrenalectomy for pheochromocytoma: morbidity compared with adrenalectomy for tumors of other pathology. J Endourol 16:245–249 (discussion 249–250)
Disclosures
Peter Nau received a Covidien Training Grant for 2008–2009. Jeffrey W. Hazey received a Stryker Research grant and a Boston Scientific Training grant, and is on the Clinical Advisory Board for Covidien and Ethicon. W. Scott Melvin is on the Advisory Board for Endogastric Solutions, Surgiquest, and Stryker. He also received training grants from Covidien and Stryker. Christopher Ellison, Vimal Narula, Peter Muscarella, and Sebastian Demyttenaere have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nau, P., Demyttenaere, S., Muscarella, P. et al. Pheochromocytoma does not increase risk in laparoscopic adrenalectomy. Surg Endosc 24, 2760–2764 (2010). https://doi.org/10.1007/s00464-010-1042-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1042-x