
Abstract
Background
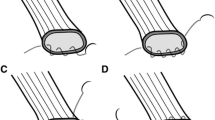
Esophagojejunostomy (EJS) represents the most difficult steps during totally laparoscopic total gastrectomy (TLTG). Over the past few years, several techniques have been developed. This study aimed to evaluate the feasibility and surgical outcomes of the laparoscopic intracorporeal side-to-side EJS during TLTG used to treat malignant disease of the stomach.
Methods
This study was conducted from June 2001 to December 2006 at three different institutions. Data were collected from patients’ medical notes, and a database was established that recorded gender, age, American Society of Anesthesiology (ASA) classification, tumor site, operative duration, time required for anastomosis, length of hospital stay, morbidity, mortality, tumor node metastasis (TNM) staging, grading, type of procedure performed, type of lymphadenectomy, conversion rate, reason for conversion, histology type, reoperation rate, reason for reoperation, time required for closure of leak, flatus time, time enteral feeding started, morbidity, and mortality.
Results
In this study, 56 totally laparoscopic gastrectomies (TLGs) (83.6%) and 11 totally laparoscopic degastrogastrectomies (TLDGs) (16.4%) with intracorporeal side-to-side EJS were performed. The average operating time was 249 min (range, 195–349 min). The average time required for both anastomoses was 44 min (17.7% of the average total time). The conversion rate was 10.4%, and the reoperation rate was 13.4%. The mean hospital stay was 12.4 days (range, 8–45 days). The major complications comprised four anastomotic leakage (6%), five postoperative bleeding (7.5%), and two duodenal stump leakage (3%). Most of the patients (91%) were enteral fed on day 6. The mean time for closure of leaks was 12 days (range, 4–18 days). The minor complications comprised two esophagojejunal anastomotic strictures (3%) subsequently treated by endoscopic dilatation. There was one death (1.5%), which occurred within 45 postoperative days.
Conclusions
Laparoscopic intracorporeal side-to-side EJS is a safe and feasible technique. It represents a valid method for performing a reconstruction of the digestive tract in laparoscopic surgery after TLG, especially in presence of a narrow esophagus.
Similar content being viewed by others


References
Azagra JS, Goergen M, De Simone P, Ibanez-Aguirre J (1999) The current role of laparoscopic surgery in the treatment of benign gastroduodenal diseases. Hepatogastroenterology 46:1522–1526
Abraham NS, Byrne CM, Young JM, Solomon MJ (2007) Metaanalysis of nonrandomized comparative studies of the short-term outcomes of laparoscopic resection for colorectal cancer ANZ J. Surg 77:508–516
Dulucq J-L, Wintringer P, Stabilini C, Solinas L, Perissat J, Mahajna A (2005) Laparoscopic and open gastric resections for malignant lesions: a prospective, comparative study. Surg Endosc 19:933–938
Goh P, Tekant Y, Kum CK, Isaac J, Ngoi SS (1992) Totally intraabdominal laparoscopic Billroth II gastrectomy. Surg Endosc 6:160
Pugliese R, Maggioni D, Sansonna F, Scandroglio I, Ferrari GC, Di Lernia S, Costanzi A, Pauna J, de Martini P (2007) Total and subtotal laparoscopic gastrectomy for adenocarcinoma. Surg Endosc 21:21–27
Asao T, Hosouchi Y, Nakabayashi T, Haga N, Mochiki E, Kuwano H (2001) Laparoscopically assisted total or distal gastrectomy with lymph node dissection for early gastric cancer. Br J Surg 88:128–132
Chau CH, Siu WT, Li MK (2002) Hand-assisted D2 subtotal gastrectomy for carcinoma of stomach. Surg Laparosc Endosc Percutan Tech 12:268–272
Huscher CG, Mingoli A, Sgarzini G, Sansonetti A, Lirici MM, Napolitano C, Piro F (2004) Videolaparoscopic total and subtotal gastrectomy with extended lynphnode dissection for gastric cancer. Am J Surg 188:728–735
Orringer MB, Marshall B, Iannettoni MD (2000) Eliminating the cervical esophagogastric anastomotic leak with a side-to-side stapled anastomosis. J Thorac Cardiovasc Surg 119:277–288
Japanese Gastric Cancer Association (1998) Japanese classification of gastric carcinoma. 2nd English edn. Gastric Cancer 1:10–24
Walther BS, Zilling T, Johnsson F, Staël von Holstein C, Joelsson B (1989) Total gastrectomy and oesophagojejunostomy with linear stapling devices. Br J Surg 76:909–912
Matsui H, Uyama I, Sugioka A, Fujita J, Komori Y, Ochiai M, Hasumi A (2002) Linear stapling forms improved anastomoses during esophagojejunostomy after a total gastrectomy. Am J Surg 184:58–60
Kim JJ, Song KY, Chin HM, Kim W, Jeon HM, Park CH, Park SM (2008) Totally laparoscopic gastrectomy with various types of intracorporeal anastomosis using laparoscopic linear staplers: preliminary experience. Surg Endosc 22:436–442
Scurtu R, Groza N, Otel O, Goia A, Funariu G (2005) Quality-of-life patients with esophagojejunal anastomosis after total gastrectomy for cancer. Rom J Gastrenterol 4:367–372
Dorsey JS, Esses S, Goldberg M, Stone R (1980) Esophagogastrestomy using the autosuture EEA surgical stapling instrument. Ann Thoracic Surg 30:308–312
Wong J, Cheung H, Lui R, Fan YW, Smith A, Siu KF (1987) Esophagogastrectomy performed with a stapler: the occurrence of leakage and stricture. Surgery 101:408–415
Fujimoto S, Takahashi M, Endoh F, Takai M, Kobayashi K, Kiuchi S, Konno C, Obata G, Okui K (1991) Stapled or manual suturing in esophagojejunostomy after total gastrectomy: a comparison of outcome in 379 patients. Am J Surg 16:256–259
West PN, Marbarger JP, Martz MN, Roper CL (1981) Esophagogastrostomy with the EEA stappler. Ann Surg 193:76–81
Nance FC (1979) New Techniques of gastrointestinal anastomoses with the EEA stapler. Ann Surg 189:587–600
Sannohe Y, Hiratsuka R, Doki K (1981) Single-layer suture by manual or mechanical stapling technique in esophagojejunostomy after total gastrectomy. Am J Surg 142:403–406
Fleming ID, Cooper JS, Henson DE et al (eds) (1997) AJCC Cancer staging manual, 5th edn. Lippincott-Raven, Philadelphia, PA
Disclosures
Umberto Bracale, Ettore Marzano, Piero Nastro, Marco Barone, Diego Cuccurullo, Giorgio Cutini, Francesco Corcione, and Giusto Pignata have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bracale, U., Marzano, E., Nastro, P. et al. Side-to-side esophagojejunostomy during totally laparoscopic total gastrectomy for malignant disease: a multicenter study. Surg Endosc 24, 2475–2479 (2010). https://doi.org/10.1007/s00464-010-0988-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-0988-z