
Abstract
Introduction
Super-morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass (LRYGB) present unique technical challenges. In our experience the ease of the operation and the operative time seem to be more dependent on body habitus than body mass index (BMI). We hypothesized that the distance between the xyphoid process and the umbilicus (the XU distance) correlated with surgical difficulty and described an original modification of trocar placement based on this measurement to improve the ease of the operation.
Methods
Seven hundred and seventy-four patients underwent LRYGB, and the XU distance was measured in a subset of 38 patients midway through the experience. The need for additional trocars was assessed intraoperatively and the relationship between the XU distance and the need for extra trocars was subsequently analyzed. A standardized approach for trocar placement was implemented in the second half of our series. The operative time was compared between the standardized and nonstandardized groups.
Results
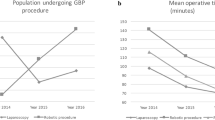
Fifty percent of the patients required a five-trocar technique. Median XU distance in this group was 21.4 cm (range 17–25 cm). In the remaining 19 patients additional trocars were added; median XU distance was 27.3 cm (range 24–33 cm). From the 774 patients included in the study period, the operative time for the first 322 patients who were completed with a nonstandardized trocar approach was significantly longer than the subsequent 452 cases in which the standardized trocar approach was used (210 versus 173 min, p < 0.001).
Conclusions
We define XU distance as the key element in determining the choice of trocar placement. When XU distance is less then 25 cm, the basic approach should be used and if it is greater than 25 cm, the advanced trocar approach is recommended. This standardized technique leads to decreased operative time and improved ease of operation.


Similar content being viewed by others


References
Shikora SA, Kim JJ, Tarnoff ME, Raskin E, Shore R (2005) Laparoscopic roux-en-y gastric bypass: results and learning curve of a high-volume academic program. Arch Surg 140:362–367
Schauer P, Ikramuddin S, Hamad G, Gourash W (2003) The learning curve for laparoscopic roux-en-y gastric bypass is 100 cases. Surg Endosc 17:212–215
Higa KD, Boone KB, Ho T, Davies OG (2000) Laparoscopic Roux-en-Y gastric bypass for morbid obesity: technique and preliminary results of our first 400 patients. Arch Surg 135:1029–1034
Higa KD, Ho T, Boone KB (2001) Laparoscopic Roux-en-Y gastric bypass: technique and 3-year follow-up. J Laparoendosc Adv Surg Techn 11:377–382
Sekhar N, Torquati A, Youssef Y, Wright JK, Richards WO (2007) A comparison of 399 open and 568 laparoscopic gastric bypasses performed during a 4-year period. Surg Endosc 21:665–668
Higa KD, Boone KB, Ho T (2000) Complications of the laparoscopic Roux-en-Y gastric bypass: 1,040 patients, what have we learned? Obes Surg 10:509–513
Campos GM, Ciovica R, Rogers SJ, Posselt AM, Vittinghoff E, Takata M, Cello JP (2007) Spectrum and risk factors of complications after gastric bypass. Arch Surg 142:969–975
Wittgrove AC, Clark GW, Tremblay LJ (1994) Laparoscopic gastric bypass, Roux-en-Y: preliminary report of five cases. Obes Surg 4:353–357
Meng WCS, Kwok SPY, Leung KL, Chung CC, Lau WY, Li AKC (1996) Optimal position of working ports in laparoscopic surgery: an in vitro study. Surg Laparosc Endosc 6:278–281
Lublin M, Lyass S, Lahmann B, Cunneen SA, Khalili TM, Elashoff JD, Phillips EH (2005) Leveling the learning curve for laparoscopic bariatric surgery. Surg Endosc 19:845–848
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Katkhouda, N., Moazzez, A., Popek, S. et al. A new and standardized approach for trocar placement in laparoscopic Roux-en-Y gastric bypass. Surg Endosc 23, 659–662 (2009). https://doi.org/10.1007/s00464-008-0075-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0075-x