
Abstract
Background
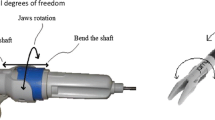
A detailed ergonomic comparison of motions and muscular activity in the left upper extremity using a laparoscopic straight or curved grasper in rectosigmoid resection is presented.
Methods
The study had two parts: experimental and clinical. In the experiment part, 30 laparoscopic sigmoid resections were performed under animal organ phantom conditions. The operations were divided into three groups according to instrument and trocar position. Group 1 (n = 10) underwent operations performed with a curved grasper in the excentral trocar position (in relation to the telescope trocar), with the left-hand curved grasper placed in the right flank and the right hand instrument in the right lower quadrant. In group 2 (n = 10), straight forceps were used in the excentral trocar position. Group 3 (n = 10) underwent laparoscopic sigmoid resection performed with a straight grasper in the central position (in relation to the telescope trocar), with the instruments placed at both sides of the lower abdomen. To measure ergonomic aspects during rectosigmoid resection, several overview video cameras, surface electromyography (EMG), an ultrasound tracking system (UTS), and a questionnaire were used. In the clinical part of the study, laparoscopic rectosigmoid resections (n = 5) were performed using a curved instrument in the excentral trocar position. The surgeon’s left-hand movement and body posture were recorded for further analysis.
Results
The curved grasper required the fewest contractions (group 1) of the measured muscles. A comparison of the UTS analysis in the experimental part of the study and the video analysis in the clinical part showed economy of movements in group 1. According to subjective estimation, both physical activity and mental stress remain at the lowest level when the excentral trocar position is used (groups 1 and 2).
Conclusions
The combination of the curved grasper and the excentral trocar position (in relation to the telescope trocar) is, according to our examinations, the best ergonomic adjustment for laparoscopic rectosigmoid surgery.

















Similar content being viewed by others


References
National Institutes of Health (1993) Consensus development conference on gallstones and laparoscopic cholecystectomy. Am J Surg 165: 390–398
Berguer R (1998) Surgical technology and the ergonomics of laparoscopic instruments. Surg Endosc 12: 458–462
Gerber S (1998) A comparative study of forces involved with manipulation of standard and laparoscopic surgical instruments [thesis]. Biomedical Engineering Program, California State University Sacramento, CA, 75 pp
Berguer R, Forkey D, Smith WD (2001) Ergonomic problems associated with laparoscopic instruments. Surg Endosc 13: 466–468
Matern U, Waller P, Giebmeyer C, Ruckauer KD, Farthmann EH (2001) Ergonomics: requirements for adjusting the height of laparoscopic operating tables. JSLS 5: 7–12
Matern U, Faist M, Kehl K, Giebmeyer C, Buess G (2005) Monitor position in laparoscopic surgery. Surg Endosc 9: 436–440
Van Veelen MA, Snijders CJ, Van Leeuwen E, Goosens RHM, Kazemier G (2003) Improvements of foot pedals used during surgery based on new ergonomic quidelines. Surg Endosc 17: 1086–1091
Uhrich ML, Underwood RA, Standeven JW, Soper NJ, Engsberg JR (2002) Assessment of fatigue monitor placement and surgical experience during simulated laparoscopic surgery. Surg Endosc 16: 635–639
Koneczny S, Matern U (2004) Instruments for the evaluation of ergonomics in the surgery. Min Invas Ther Allied Technol 13: 167–177
Delagi EF, Iazzetty J, Perotto A, Morrison D (1980) Anatomic guide for the electromyographer. Charles S. Thomas, Springfield, IL
Konrad K (2005) The ABC of EMG: a practical introduction to kinesiological electromyography
Dwivedi A, Chahin F, Agrawal S, Chau WY, Tootla A, Tootla F, Silva YJ (2002) Laparoscopic colectomy vs open colectomy for sigmoid diverticular disease. Dis Colon Rectum 45: 1309–1315
Eijsbouts QAJ, de Haan J, Berends F, Sietses C, Cuesta MA (2000) Laparoscopic elective treatment of diverticular disease: a comparison between laparoscopic-assisted and resection-facilitated techniques. Surg Endosc 14: 726–730
Schwandner O, Farke S, Bruch H-P (2005) Laparoscopic colectomy for diverticulitis is not associated with increased morbidity when compared with nondiverticular disease. Int J Colorectal Dis 20: 165–172
Tuech J-J, Pessaux P, Rouge C, Regenet N, Bergamaschi R, Arnaud J-P (2000) Laparoscopic vs open colectomy for sigmoid diverticulitis: a prospective comparative study in the elderly. Surg Endosc 14: 1031–1033
Dincler S, Koller MT, Steurer J, Bachmann LM, Christen D, Buchmann P (2003) Multidimensional analysis of learning curves in laparoscopic sigmoid resection: eight-year results. Dis Colon Rectum 46: 1371–1379
Smadja C, Sbai IM, Tahrat M, Vons C, Bobocescu E, Baillet P, Franco D (1999) Elective laparoscopic sigmoid colectomy for diverticulitis: results of a prospective study. Surg Endosc 13: 645–648
Tuech J-J, Regenet N, Hennekinne S, Pessaux P, Bergamaschi R, Arnaud J-P (2001) Laparoscopic colectomy for sigmoid diverticulitis in obese and nonobese patients: a prospective comparative study. Surg Endosc 15: 1427–1430
Koeckerling F, Schneider C, Reymond MA, Scheidbach H, Scheuerlein H, Konradt J, Bruch HP, Zornig C, Koehler L, Baerlehner E, Kuthe A, Szinicz G, Richter HA, Hohenberger W, Laparoscopic Colorectal Surgery Study Group (1999) Laparoscopic resection of sigmoid diverticulitis: results of a multicenter study. Surg Endosc 13: 567–571
Scheidbach H, Schneider C, Rose J, Konradt J, Gross E, Bärlehner E, Pross M, Schmidt U, Köckerling F, Lippert H (2004) Laparoscopic approach to treatment of sigmoid diverticulitis: changes in the spectrum of indications and results of a prospective, multicenter study on 1,545 patients. Dis Colon Rectum 47: 1883–1888
Hanna GB, Shimi S, Cuschieri A (1997) Optimal port locations for endoscopic intracorporeal knotting. Surg Endosc 11: 397–401
Goossens RHM, van Veelen MA (2001) Assessment of ergonomics in laparoscopic surgery. Min Invas Ther Allied Technol 10: 175–179
Hoolhorst FWB (2005) Design of a handle for curved instruments [master thesis]. Section for Minimally Invasive Surgery, University Clinic of General, Visceral and Transplantation Surgery. Tuebingen, Germany, 107 pp
Johnsson B (1978) Quantitative electromyographic evaluation of muscular load during work. Scand J Rehabil Med 6: 69–74
Acknowledgments
This research was sponsored by Alexander von Humboldt fellowship.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Manukyan, G.A., Waseda, M., Inaki, N. et al. Ergonomics with the use of curved versus straight laparoscopic graspers during rectosigmoid resection: results of a multiprofile comparative study. Surg Endosc 21, 1079–1089 (2007). https://doi.org/10.1007/s00464-007-9284-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9284-y