
Abstract
Background
This randomized trial compared thoracic epidural analgesia with patient-controlled analgesia (PCA) using morphine for laparoscopic colectomy in a traditional, nonaccelerated, perioperative care program.
Methods
In the study, 50 patients scheduled for elective laparoscopic colon resection were randomized to either PCA morphine (n = 25) or thoracic epidural analgesia with bupivacaine and fentanyl (n = 25). Both groups received general anesthesia and multimodal pain relief, which included naproxen and acetaminophen for as long as 4 postoperative days. Time until passage of gas and bowel movements, dietary intake, postoperative quality of analgesia, readiness for discharge, and length of hospital stay were recorded.
Results
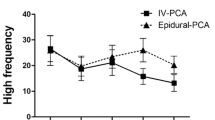
Recovery of postoperative ileus occurred sooner in the epidural group (p < 0.005) by an average 1 to 2 days, and resumption of full diet was achieved earlier (p < 0.05). Intensity of pain during the first 2 postoperative days was significantly lower at rest, with coughing, and with walking in the epidural group (p < 0.005). Readiness for discharge and hospital length of stay (5 days) were otherwise similar in the two groups.
Conclusions
When a traditional perioperative care program is used for laparoscopic colectomy, thoracic epidural analgesia is superior to PCA in accelerating the return of bowel function and dietary intake, while providing better pain relief.
Similar content being viewed by others

References
Abraham NS, Young JM, Solomon MJ (2004) Meta-analysis of short-term outcomes after laparoscopic resection for colorectal cancer. Br J Surg 91: 1111–1124
Hildebrabdt U, Kessler K, Plusczyk T, Pistorius C, Vollmar B, Menger MD (2002) Comparison of surgical stress between laparoscopic and open colonic resections. Surg Endosc 17: 242–246
Carli F, Galeone M, Gzodic B, Hong X, Fried GM, Wykes L, Eberhart L, Schricker T (2005) Laparoscopic colon resection improves postoperative glucose utilization without protein-sparing effect. Arch Surg 140: 593–597
Kehlet H (2002) Clinical trials and laparoscopic surgery. Surg Laparosc Endosc 12: 137–138
Wilmore DW, Kehlet H (2001) Management of patients in fast-track surgery. BMJ 322: 473–476
Basse L, Hjort Jakobsen S, Billesbolle P, Werner M, Kehlet H (2000) A clinical pathway to accelerate recovery after colonic resection. Ann Surg 232: 51–57
Basse L, Jakobsen DH, Bardram L, Billesbolle P, Lund C, Mogesen T, Rosemberg J, Kehlet H (2005) Functional recovery after open versus laparoscopic colonic resection. Ann Surg 241: 416–423
Kehlet H, Wilmore DW (2005) Fast-track surgery. Br J Surg 92: 3–4
Liu S (2004) Anesthesia and analgesia for colon surgery. Reg Anesth Pain Med 29: 52–57
Carli F, Trudel J, Belliveau P (2001) The effect of intraoperative thoracic epidural anesthesia and postoperative analgesia on bowel function after colorectal surgery. Dis Colon Rectum 44: 1083–1089
Neudecker J, Schwenk W, Junghans T, Pietsch S, Bohm B, Muller JM (1999) Randomized controlled trial to examine the influence of thoracic epidural analgesia on postoperative ileus after laparoscopic sigmoid resection. Br J Surg 86: 1292–1295
Senagore AJ, Whalley D, Delaney CP, Mekhail N, Duepree HJ, Fazio VW (2001) Epidural anesthesia-analgesia shortens length of stay after laparoscopic segmental colectomy for benign pathology. Surgery 129: 672–676
Kehlet H, Holte K (2001) Review of postoperative ileus. Am J Surg 182: 3S–10S
The Clinical Outcomes of Surgical Therapy Study Group (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. New Engl J Med 350: 2050–2059
Lacy AM, Garcia-Valdecasas JC, Delgado S, Castells A, Taura P, Pique JM, Visa J (2002) Laparoscopic-assisted colectomy versus open colectomy for treatment of nonmetastatic colon cancer: a randomized trial. Lancet 359: 2224–2229
Leroy J Jamali F, Forbes L, Smith M, Rubino F, Mutter D, Marescaux J (2004) Laparoscopic total mesorectal excision (TME) for colorectal cancer: long-term outcomes. Surg Endosc 18: 281–289
Bardram L, Funch-Jensen P, Gensen P, Crawford ME, Kehlet H (1995) Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobilization. Lancet 345: 763–764
Senagore AJ, Delaney CP, Mekhail N, Dgan A, Fazio VW (2003) Randomized clinical trial comparing epidural anaesthesia and patient-controlled analgesia after laparoscopic segmental colectomy. Br J Surg 90: 1195–1199
Zutshi M, Delaney C, Senagore AJ, Mekhail N, Lewis B, Connor JT, Fazio VW (2005) Randomized controlled trial comparing the controlled rehabilitation with early ambulation and diet pathway versus the controlled rehabilitation with early ambulation and diet with preemptive epidural anesthesia/analgesia after laparotomy and intestinal resection. Am J Surg 189: 268–272
Carli F, Kehlet H (2005) Continuous epidural analgesia for colonic surgery: but what about the future? Reg Anesth Pain Med 30: 140–142
Carli F, Mayo N (2001) Measuring the outcome of surgical procedures: what are the challenges? Br J Anaesth 87: 531–533
Acknowledgments
Dr. X. Hong was awarded a fellowship from the McGill University Health Centre (MUHC) Foundation. Dr. G. Mistraletti was the recipient of a scholarship from the University of Milan and the Societa’ Italiana di Anestesia, Rianimazione e Terapia Intensiva (SIARTI). An operating grant for this project was provided by the MUHC Research Institute to Dr. F Carli.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Taqi, A., Hong, X., Mistraletti, G. et al. Thoracic epidural analgesia facilitates the restoration of bowel function and dietary intake in patients undergoing laparoscopic colon resection using a traditional, nonaccelerated, perioperative care program. Surg Endosc 21, 247–252 (2007). https://doi.org/10.1007/s00464-006-0069-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-006-0069-5