
Abstract
Background
Percutaneous endoscopic gastrostomy (PEG) has been an invaluable method for obtaining long-term enteral access and represents one of the first forays in the field of minimally invasive surgery. However, the traditional “pull” method for PEG tube placement continues to have some disadvantages, especially in patients with near-obstructive head and neck cancers.
Methods
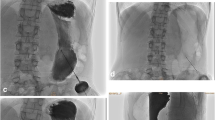
We describe a new “SLiC” technique for establishing percutaneous gastrostomy using a radially expandable trocar.
Results
This technique is initially developed and refined on a porcine model and then successfully implemented on five human patients.
Conclusion
The SLiC technique can be done safely and efficiently with a pediatric-sized gastroscope and avoids the need for radiation from fluoroscopy. It is a good alternative for obtaining enteral access in patients who would otherwise not be well suited for a traditional PEG tube.










Similar content being viewed by others


References
Adelson RT, Ducic Y (2005) Metastatic head and neck carcinoma to a percutaneous endoscopic gastrostomy site. Head Neck 27: 339–343
Bhama JK, Haas MK, Fisher WE (2001) Spread of a pharyngeal cancer to the abdominal wall after percutaneous endoscopic gastrostomy. Surg Laparosc Endosc Percutan Tech 11: 375–378
Felsher J, Chand B, Ponsky J (2004) Decompressive percutaneous endoscopic gastrostomy in nonmalignant disease. Am J Surg 187: 254–256
Foutch PG, Talbert GA, Waring JP, Sanowski RA (1988) Percutaneous endoscopic gastrostomy in patients with prior abdominal surgery: virtues of the safe tract. Am J Gastroenterol 83: 147–150
Gauderer MW, Ponsky JL, Izant RJ Jr (1980) Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg 15: 872–875
Laccourreye O, Chabardes E, Merite-Drancy A, Carnot F, Renard P, Donnadieu S, Brasnu D (1993) Implantation metastasis following percutaneous endoscopic gastrostomy. J Laryngol Otol 107: 946–949
Larson DE, Burton DD, Schroeder KW, DiMagno EP (1987) Percutaneous endoscopic gastrostomy. Indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology 93: 48–52
Lee DS, Mohit-Tabatabai MA, Rush BF Jr, Levine C (1995) Stomal seeding of head and neck cancer by percutaneous endoscopic gastrostomy tube placement. Ann Surg Oncol 2: 170–173
Maccabee D, Sheppard BC (2003) Prevention of percutaneous endoscopic gastrostomy stoma metastases in patients with active oropharyngeal malignancy. Surg Endosc 17: 1678
Meurer MF, Kenady DE (1993) Metastatic head and neck carcinoma in a percutaneous gastrostomy site. Head Neck 15: 70–73
Peghini PL, Guaouguaou N, Salcedo JA, Al-Kawas FH (2000) Implantation metastasis after PEG: case report and review. Gastrointest Endosc 51: 480–482
Ponsky JL, (2004) Percutaneous endoscopic gastrostomy. J Gastrointest Surg 8: 903–906
Ponsky JL, Gauderer MW (1981) Percutaneous endoscopic gastrostomy: a nonoperative technique for feeding gastrostomy. Gastrointest Endosc 27: 9–11
Ponsky JL, Gauderer MW, Stellato TA (1983) Percutaneous endoscopic gastrostomy. Review of 150 cases. Arch Surg 118: 913–914
Pothuri B, Montemarano M, Gerardi M, Shike M, Ben-Porat L, Sabbatini P, Barakat RR (2005) Percutaneous endoscopic gastrostomy tube placement in patients with malignant bowel obstruction due to ovarian carcinoma. Gynecol Oncol 96: 330–334
Righi PD, Reddy DK, Weisberger EC, Johnson MS, Trerotola SO, Radpour S, Johnson PE, Stevens CE (1998) Radiologic percutaneous gastrostomy: results in 56 patients with head and neck cancer. Laryngoscope 108: 1020–1024
Ruppin H, Lux G (1986) Percutaneous endoscopic gastrostomy in patients with head and neck cancer. Endoscopy 18: 149–152
Russell TR, Brotman M, Norris F (1984) Percutaneous gastrostomy. A new simplified and cost-effective technique. Am J Surg 148: 132–137
Sacks BA, Vine HS, Palestrant AM, Ellison HP, Shropshire D, Lowe R (1983) A nonoperative technique for establishment of a gastrostomy in the dog. Invest Radiol 18: 485–487
Scott JS, de la Torre RA, Unger SW (1991) Comparison of operative versus percutaneous endoscopic gastrostomy tube placement in the elderly. Am Surg 57: 338–340
Sinclair JJ, Scolapio JS, Stark ME, Hinder RA (2001) Metastasis of head and neck carcinoma to the site of percutaneous endoscopic gastrostomy: case report and literature review. J Parenter Enteral Nutr 25: 282–285
Thompson WM, Oddson TA, Kelvin F, Daffner R, Postlethwait RW, Rice RP (1978) Synchronous and metachronous squamous cell carcinomas of the head, neck and esophagus. Gastrointest Radiol 3: 123–127
Thorburn D, Karim SN, Soutar DS, Mills PR (1997) Tumour seeding following percutaneous endoscopic gastrostomy placement in head and neck cancer. Postgrad Med J 73: 430–432
Tucker AT, Gourin CG, Ghegan MD, Porubsky ES, Martindale RG, Terris DJ (2003) ‘Push’ versus ‘pull’ percutaneous endoscopic gastrostomy tube placement in patients with advanced head and neck cancer. Laryngoscope 113: 1898–1902
Weaver A, Fleming SM, Knechtges TC, Smith D (1979) Triple endoscopy: a neglected essential in head and neck cancer. Surgery 86: 493–496
Yip D, Vanasco M, Funaki B (2004) Complication rates and patency of radiologically guided mushroom gastrostomy, balloon gastrostomy, and gastrojejunostomy: a review of 250 procedures. Cardiovasc Intervent Radiol 27: 3–8
Zhou YQ, Li XM, Gao CM, Zhao QL, Li GS, Cheng JM, Shang YD (2004) [Clinical analysis of 71 cases of multiple primary cancers in head and neck squamous carcinomas]. Zhonghua Er Bi Yan Hou Ke Za Zhi 39: 232–236
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sabnis, A., Liu, R., Chand, B. et al. SLiC technique. Surg Endosc 20, 256–262 (2006). https://doi.org/10.1007/s00464-005-0383-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0383-3