
Abstract
Purpose
Erlotinib is indicated as first-line treatment for patients with non-small-cell lung cancer (NSCLC) harboring an epidermal growth-factor–receptor (EGFR) mutation. Addition of a vascular endothelial growth factor (VEGF) inhibitor (anti-VEGF) in combination with the tyrosine-kinase inhibitor erlotinib in this setting is controversial.
Methods
We conducted a meta-analysis of randomized trials comparing anti-VEGF plus erlotinib vs erlotinib alone as first-line therapy for advanced NSCLC harboring an EGFR mutation. Outcomes included overall survival (OS), progression-free survival (PFS), objective response rate (ORR) and median duration of response (DOR). A fixed-effect model was used.
Results
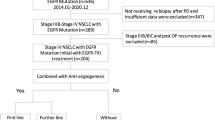
Four studies evaluated bevacizumab + erlotinib (ARTEMIS, NEJ026, J025667, Stinchcombe et al.), and another evaluated ramucirumab + erlotinib (RELAY). These five eligible studies included 1230 non-squamous NSCLC patients, 654 (53.2%) with exon 19 deletion (ex19del) and 568 (46.8%) with EGFRL858R. Patients were predominantly women (63%), Asians (85%) and non-smokers (60%); the median age was 64 years. The combination (anti-VEGF + erlotinib) was significantly associated with prolonged PFS (hazards ratio [HR] 0.59 [95% confidence interval (CI) 0.51–0.69]; p < 0.00001). The combination achieved significantly longer median DOR (p < 0.005). Based on interim analyses, OS (HR 0.90 [0.68–1.19]; p = 0.45) and ORR (odds ratio 1.19 [95% CI 0.91–1.55]; p = 0.21 were comparable.
Conclusions
For patients with untreated, advanced, EGFR-mutation–harboring NSCLCs, the anti-VEGF + erlotinib combination, compared to erlotinib alone, was associated with significantly prolonged PFS but mature data for OS are needed to confirm the benefit of this strategy.




Similar content being viewed by others


References
Akamatsu H, Koh Y, Ozawa Y, Fujimoto D, Hata A, Katakami N, Tomii K, Shimokawa T, Yamamoto N (2018) Osimertinib with Ramucirumab in EGFR-mutated, T790M-positive patients with progression during EGFR-TKI therapy: phase Ib study. Clin Lung Cancer 19(6):e871–e874. https://doi.org/10.1016/j.cllc.2018.08.001
Akamatsu H, Teraoka S, Morita S, Katakami N, Tachihara M, Daga H, Yamamoto N, Nakagawa K (8715L) Phase I/II Study of Osimertinib With Bevacizumab in EGFR-mutated, T790M-positive patients with progressed EGFR-TKIs: West Japan Oncology Group 8715L (WJOG8715L). Clin Lung Cancer 20(4):e492–e494. https://doi.org/10.1016/j.cllc.2019.03.002
Castellanos E, Feld E, Horn L (2017) Driven by mutations: the predictive value of mutation subtype in EGFR-mutated non-small cell lung cancer. J Thoracic Oncol 12(4):612–623. https://doi.org/10.1016/j.jtho.2016.12.014
Gridelli C, Rossi A, Ciardiello F, De Marinis F, Crinò L, Morabito A, Morgillo F et al (2016) BEVERLY: rationale and design of a randomized open-label phase III trial comparing bevacizumab plus erlotinib vs erlotinib alone as first-line treatment of patients with EGFR-mutated advanced nonsquamous non-small-cell lung cancer. Clin Lung Cancer 17(5):461–465. https://doi.org/10.1016/j.cllc.2016.04.001
Herbst RS, Ansari R, Bustin F, Flynn P, Hart L, Otterson GA, Vlahovic G, Soh C-H, O’Connor P, Hainsworth J (2011) Efficacy of bevacizumab plus erlotinib vs erlotinib alone in advanced non-small-cell lung cancer after failure of standard first-line chemotherapy (BeTa): a double-blind, placebo-controlled, phase 3 trial. Lancet (London, England) 377(9780):1846–1854. https://doi.org/10.1016/S0140-6736(11)60545-X
Kitagawa C, Kada A, Saito AM, Ichinose Y, Saka H (2019) Rationale and design of a randomized phase 2 trial of gefitinib plus bevacizumab vs gefitinib alone in patients with epidermal growth factor receptor mutant non-squamous non-small-cell lung cancer: study protocol. Kurume Med J 65(2):77–81. https://doi.org/10.2739/kurumemedj.MS652001
Li X-Y, Lin J-Z, Shu-Han Yu (2020) Front-line therapy in advanced non-small cell lung cancer with sensitive epidermal growth factor receptor mutations: a network meta-analysis. Clin Ther. https://doi.org/10.1016/j.clinthera.2019.12.006
Maemondo M, Tatsuro F, Haruhiro S, Naoki F, Kana W, Shunichi S, Shunichiro I et al (2020) NEJ026: final overall survival analysis of bevacizumab plus erlotinib treatment for NSCLC patients harboring activating EGFR-mutations. J Clin Oncol 38(15):9506–9506. https://doi.org/10.1200/JCO.2020.38.15_suppl.9506
Nakagawa K, Edward BG, Takashi S, Makoto N, Santiago PA, Luis P-A, Chao HC et al (2019) Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. https://doi.org/10.1016/S1470-2045(19)30634-5
Ninomiya T, Ishikawa N, Inoue K, Kubo T, Yasugi M, Shibayama T, Maeda T et al (2019) Phase 2 study of afatinib alone or combined with bevacizumab in chemonaive patients with advanced non-small-cell lung cancer harboring EGFR mutations: AfaBev-CS study protocol. Clin Lung Cancer 20(2):134–138. https://doi.org/10.1016/j.cllc.2018.10.008
Ramalingam SS, Vansteenkiste J, Planchard D, Cho BC, Gray JE, Ohe Y, Zhou C et al (2020) Overall survival with Osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med 382(1):41–50. https://doi.org/10.1056/NEJMoa1913662
Rosell R, Dafni U, Felip E, Curioni-Fontecedro A, Gautschi O, Peters S, Massutí B et al (2017) Erlotinib and bevacizumab in patients with advanced non-small-cell lung cancer and activating EGFR mutations (BELIEF): an international, multicentre, single-arm, phase 2 trial. Lancet Respir Med 5(5):435–444. https://doi.org/10.1016/S2213-2600(17)30129-7
Saito H, Fukuhara T, Furuya N, Watanabe K, Sugawara S, Iwasawa S, Tsunezuka Y et al (2019) Erlotinib plus bevacizumab vs erlotinib alone in patients with EGFR-positive advanced non-squamous non-small-cell lung cancer (NEJ026): interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol 20(5):625–635. https://doi.org/10.1016/S1470-2045(19)30035-X
Seto T, Kato T, Nishio M, Goto K, Atagi S, Hosomi Y, Yamamoto N et al (2014) Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol 15(11):1236–1244. https://doi.org/10.1016/S1470-2045(14)70381-X
Soria J-C, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, Dechaphunkul A et al (2018) Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Eng J Med 378(2):113–125. https://doi.org/10.1056/NEJMoa1713137
Stinchcombe TE, Jänne PA, Wang X, Bertino EM, Weiss J, Bazhenova L, Lin Gu et al (2019) Effect of erlotinib plus bevacizumab vs erlotinib alone on progression-free survival in patients with advanced EGFR-mutant non-small cell lung cancer: a phase 2 randomized clinical trial. JAMA Oncol. https://doi.org/10.1001/jamaoncol.2019.1847
Wu Y-L, Cheng Y, Zhou X, Lee KH, Nakagawa K, Niho S, Tsuji F et al (2017) Dacomitinib vs gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol 18(11):1454–1466. https://doi.org/10.1016/S1470-2045(17)30608-3
Zhang S, Mao X-D, Wang H-T, Cai F, Jing Xu (2016) Efficacy and safety of bevacizumab plus erlotinib vs bevacizumab or erlotinib alone in the treatment of non-small-cell lung cancer: a systematic review and meta-analysis. BMJ Open 6(6):e011714. https://doi.org/10.1136/bmjopen-2016-011714
Zhao B, Zhang W, Dongliang Yu, Jianjun Xu, Wei Y (2018) Erlotinib in combination with bevacizumab has potential benefit in non-small cell lung cancer: a systematic review and meta-analysis of randomized clinical trials. Lung Cancer (Amsterdam, Netherlands) 122:10–21. https://doi.org/10.1016/j.lungcan.2018.05.011
Zhou Q, Wu Y-L, Cheng Y, Liu Y, Chen G, Cui J, Yang N et al (1480OCTONG) 1480OCTONG 1509: Phase III study of bevacizumab with or without erlotinib in untreated chinese patients with advanced EGFR-mutated NSCLC. Ann Oncol. https://doi.org/10.1093/annonc/mdz260.002
Zhou K, Zhao S, Guo W, Ding L (2020) Efficacy and safety of erlotinib combined with bevacizumab in the treatment of non-small cell lung cancer: a systematic review and meta-analysis. Medicine 99(3):e18771. https://doi.org/10.1097/MD.0000000000018771
Funding
Academic funding by OREP (organization pour la recherche en Pneumologie).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
JBA was supported by grants from Fondation pour la Recherche Médicale (FRM). CC reports consultancy fees from Astra Zeneca, Boehringer Ingelheim, MSD, Pierre Fabre Oncology, Lilly, Roche, Bristol- Myers Squibb, Novartis, Lilly, Pierre Fabre Oncology and Boehringer Ingelheim.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Landre, T., Des Guetz, G., Chouahnia, K. et al. First-line angiogenesis inhibitor plus erlotinib versus erlotinib alone for advanced non-small-cell lung cancer harboring an EGFR mutation. J Cancer Res Clin Oncol 146, 3333–3339 (2020). https://doi.org/10.1007/s00432-020-03311-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-020-03311-w