
Abstract
Background
The purpose of the current study is to evaluate the efficacy and complications of concurrent chemoradiotherapy (CCRT) for the treatment of gastric cancer patients after D1/D2 surgery.
Methods
Sixty-eight untreated gastric cancer patients (T3/T4 and/or N+) were enrolled. After surgery, they were randomized into two groups: the CCRT group and the single chemotherapy group. Radiotherapy patients were treated according to the Intergroup 0116 guidelines. The chemotherapy consisted of continuously administered 5-fluorouracil (5-FU) and tetrahydrofolic acid (LV). The CCRT began 28 days after the first cycle of chemotherapy, and chemotherapy was given within the first four and last three days during the CCRT period, at a radiation dosage of 45 Gy/25 f, i.e., 1.8 Gy 5 times per week. Two cycles of the same chemotherapy were administrated 1 month after the radiotherapy. Five cycles of 5-FU and LV were applied to CG.
Results
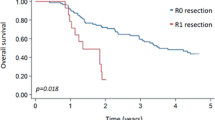
One-, two-, and three-year survival rates were 85.9, 73.4, and 67.7%, respectively, in the CCRT group and 68.0, 50.0, and 44.1%, in the single chemotherapy group (P < 0.05). The corresponding disease-free survival rates were 73.5, 64.7, and 55.8% in the CCRT group and 61.8, 38.2, and 29.4% in the single chemotherapy group (P < 0.05). The major side effects were gastrointestinal reactions and neutrocytopenia. In both the CCRT and single chemotherapy groups, the incidence of these side effects was 73.5% (25/34) and 44.1% (15/34) (P < 0.05) for Grade I and Grade II anorexia, 82.35% (28/34) and 73.5% (25/34) (P > 0.05) for nausea and vomiting, and 70.6% (24/34) and 44.1% (15/34) (P < 0.05) for neutrocytopenia, respectively. The other indices showed no significant differences.
Conclusions
Our findings indicate that CCRT can increase the one-, two-, and three-year total survival rates, as well as the disease-free survival rates of gastric cancer patients (T3/T4 and/or N+) who have been initially treated with surgery. The major adverse reactions were Grade I and Grade II nausea and vomiting, as well as myelosuppression. CCRT is well tolerated.


Similar content being viewed by others


References
Coburn NG, Guller U, Baxter NN, Kiss A, Ringash J, Swallow CJ, Law CH (2008) Adjuvant therapy for resected gastric cancer–rapid, yet incomplete adoption following results of intergroup 0116 trial. Int J Radiat Oncol Biol Phys 70:1073–1080
Fiorica F, Cartei F, Enea M, Licata A, Cabibbo G, Carau B, Liboni A, Ursino S, Camma C (2007) The impact of radiotherapy on survival in resectable gastric carcinoma: a meta-analysis of literature data. Cancer Treat Rev 33:729–740
Hartgrink HH, van de Velde CJ (2005) Status of extended lymph node dissection: locoregional control is the only way to survive gastric cancer. J Surg Oncol 90:153–165
Jansen EP, Saunders MP, Boot H, Oppedijk V, Dubbelman R, Porritt B, Cats A, Stroom J, Valdes OR, Bartelink H, Verheij M (2007) Prospective study on late renal toxicity following postoperative chemoradiotherapy in gastric cancer. Int J Radiat Oncol Biol Phys 67:781–785
Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, Thun MJ (2006) Cancer statistics. CA Cancer J Clin 56:106–130
Kim S, Lim DH, Lee J, Kang WK, MacDonald JS, Park CH, Park SH, Lee SH, Kim K, Park JO, Kim WS, Jung CW, Park YS, Im YH, Sohn TS, Noh JH, Heo JS, Kim YI, Park CK, Park K (2005) An observational study suggesting clinical benefit for adjuvant postoperative chemoradiation in a population of over 500 cases after gastric resection with D2 nodal dissection for adenocarcinoma of the stomach. Int J Radiat Oncol Biol Phys 63:1279–1285
Kozak KR, Moody JS (2008) The survival impact of the intergroup 0116 trial on patients with gastric cancer. Int J Radiat Oncol Biol Phys 72:517–521
Lim DH, Kim DY, Kang MK, Kim YI, Kang WK, Park CK, Kim S, Noh JH, Joh JW, Choi SH, Sohn TS, HeoJS Park CH, Park JO, Lee JE, Park YJ, Nam HR, Park W, Ahn YC, Huh SJ (2004) Patterns of failure in gastric carcinoma after D2 gastrectomy and chemoradiotherapy: a radiation oncologist’s view. Br J Cancer 91:11–17
Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA (2001) Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 345:725–730
Milano MT, Garofalo MC, Chmura SJ, Farrey K, Rash C, Heimann R, Jani AB (2006) Intensity-modulated radiation therapy in the treatment of gastric cancer: early clinical outcome and dosimetric comparison with conventional techniques. Br J Radiol 79:497–503
Roukos DH, Kappas AM (2005) Perspectives in the treatment of gastric cancer. Nat Clin Pract Oncol 2:98–107
Acknowledgments
We would like to thank the staff in the department of Gastroenterology, CT Medical Imaging, Medical Record, and Tumor Radiotherapy for their assistance.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yu, C., Yu, R., Zhu, W. et al. Intensity-modulated radiotherapy combined with chemotherapy for the treatment of gastric cancer patients after standard D1/D2 surgery. J Cancer Res Clin Oncol 138, 255–259 (2012). https://doi.org/10.1007/s00432-011-1085-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-011-1085-y