
Abstract
Background
Bendamustine is an alkylator with anticipated antimetabolic activity. It has shown activity in malignant lymphoma, multiple myeloma, and breast cancer. Recognized side-effects are relatively mild with myelosuppression as the dose-limiting toxicity. The CD4/CD8 ratio may be reduced. To what extent the alteration of lymphocytes, especially CD4+ lymphocytes, correlates with an increase in opportunistic infections cannot be definitively answered.
Case report
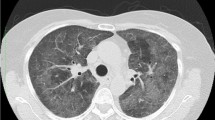
The patient, female, aged 48 years, was suffering from an advanced progressive breast cancer. After initial treatment with several chemotherapies, a cytotoxic therapy was initiated, with bendamustine (150 mg/m2) administered on two consecutive days and repeated every 4 weeks. After five courses, the patient developed Pneumocystis carinii pneumonia (PCP), disclosed in the bronchoalveolar lavage. While receiving bendamustine therapy, the CD4+ and CD8+ lymphocyte counts in the peripheral blood were determined by flow cytometry. The next-to-normal CD4/CD8 ratio before therapy (0,82) had decreased to 0,05 during the therapy mainly due to a decline of CD4+ lymphocyte. The patient was seronegative for human immunodeficiency virus. In spite of high-dose intravenous trimethoprim/sulfamethoxazole and methylprednisolone application, the patient died of a respiratory failure 3 days after PCP was diagnosed.
Conclusion
Bendamustine is capable of inducing a reduction in CD4+ lymphocyte counts causing a severe T-lymphocyte-mediated immunosuppression. Measuring CD4+ lymphocyte counts may be helpful in determining the risk of PCP in patients treated with bendamustine.


Similar content being viewed by others


References
Strumberg D, Harstrick A, Doll K, et al (1996) Bendamustine hydrochloride activity against doxorubicine-resistant human breast carcinoma cell lines. Anti Cancer Drugs 7:415–421
Reck M, Haering B, Koschel G, et al (1998) Chemotherapie des fortgeschrittenen nicht-kleinzelligen und kleinzelligen Bronchialkarzinoms mit Bendamustin—Eine Phase-II-Studie. Pneumologie 52:571–574
Rahn AN, Schilcher RB, Adamietz IA, et al (2001) Palliative Radiochemotherapie mit Bendamustin bei fortgeschrittenen Tumorrezidiven im HNO-Bereich. Strahlenther Onkol 177:189–194
Bremer K, Roth W (1996) Bendamustine, a low-toxic nitrogen-mustard derivative with high efficacy in malignant lymphomas. Tumordiagn Ther 17:1–6
Matthias M, Preiss R, Sohr R, Possinger K (1995) Pharmakokinetics of bendamustine in patients with malignant tumors. Proc Am Assoc Clin Oncol 14:458 [abstr]
Höffken K, Merkle Kh, Schönfelder M, et al (1998) Bendamustine as salvage treatment in patients with advanced progressive breast cancer:a phase II study. J Cancer Res Clin Oncol 124:627–632
Schöffski P, Hagedorn T, Grünwald V, et al (2000) Repeated administration of short infusions of bendamustine: a phase I study in patients with advanced progressive solid tumours. J Cancer Res Clin Oncol 126:41–47
Schöffski P, Seeland G, Engel H, et al (2000) Weekly administration of bendamustine: a phase I study in patients with advanced progressive solid tumours. Ann Oncol 11:729–734
Kath R, Blumenstengel K, Fricke HJ, Höffken K (2001) Bendamustine monotherapy in advanced and refractory chronic lymphocytic leukemia. J Cancer Res Clin Oncol 127:48–54
Wijermans PW, Gerrits WB, Haak HL (1993) Severe immunodeficiency in patients treated with fludarabine monophosphate. Eur J Haematol 50:292–296
Bastie JN, Cazals-Hatem D, Daniel MT, et al (1999) Five years follow-up after 2-chlorodeoxyadenosine treatment in thirty patients with hairy cell leukemia: evaluation of minimal residual disease and CD4+lymphocytopenia after treatment. Leuk Lymphoma 35:555–565
Kath R, Blumenstengel K, Fricke HJ, et al (2001) Bendamustin, Vincristin, Prednisolon (BOP) in der Therapie von fortgeschrittenen niedrig malignen Non-Hodgkin-Lymphomen. Dtsch med Wschr 126:198–202
Ruffert K, Jahn H, Jorke D (1988) A comparative study of cytostasan, methotrexate (MTX) plus fluorouracil (5-FU) and CMF in advanced breast cancer (abstract). Proc Eur Soc Med Oncol 240
Brockmann B, Kirchhof I, Geschke E, Schmidt UM (1989) Therapieergebnisse und toxische Nebenwirkungen der Kombination Cytostasan, Adriamycin und Vincristin als "second line"-Therapie beim metastasierenden Mammakarzinom. Arch Geschwulstforsch 59:341–346
Sayer HG, Vogt T, Hoffmann K, Wollina K, Mügge LO, Höffken K (2000) High response-rate of short duration with a double high-dose-chemotherapy regimen of doxorubicin/paclitaxel/cyclophosphamide/thiotepa [ATCT] and peripheral blood progenitor cell support in patients with metastatic breast cancer. Bone Marrow Transplantation 26[Suppl 1]:S 34
Schadeck-Gressel C, Eberhardt B, Westerhausen M (1998) Bendamustine as immune suppressive agent in five cases of therapy refractory autoimmune thrombocytopenic purpura (ITP). Proc Am Soc Clin Oncol 18:18a [abstr 65]
Siminski J, Kidd P, Phillips GD (1991) Reversed helper/suppressor T-lymphocyte ratio in bronchoalveolar lavage from patients with breast cancer and Pneumocystis carinii Pneumonia. Am Rev Respir Dis 143:437–440
Kane GC, Troshinsky MB, Peters SP, Israel HL (1993) Pneumocystis carinii pneumonia associated with weekly methotrexate: cumulative dose of methotrexate and low CD4 cell count may predict this complication. Respir Med 87:153–155
Phair J, Munoz A, Detels R, et al (1990) The risk of Pneumocystis carinii pneumonia among men infected with human immundeficiency virus type 1. Multicenter AIDS cohort study group. N Engl J Med 322:161–165
Glück T, Geerdes-Fenge HF, Straub RH, et al (2000) Pneumocystis carinii Pneumonia as acomplication of immunsuppressive therapy. Infection 28:227–230
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Klippstein, A., Schneider, C.P., Sayer, H.G. et al. Pneumocystis carinii pneumonia as a complication of bendamustine monotherapy in a patient with advanced progressive breast cancer. J Cancer Res Clin Oncol 129, 316–319 (2003). https://doi.org/10.1007/s00432-003-0441-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-003-0441-y